Older Americans prefer to remain in their current dwellings as long as possible and usually move infrequently, that is, they age in place. This paper explains their infrequent relocation adjustments and shows that this residential inertia results in significant shares of older people who live in unaffordable dwellings with physical deficiencies, in neighborhoods with various undesirable physical and social changes, and who are socially isolated with unmet long-term care needs. To account for this residential inertia despite these problems, it is necessary to understand the strong attractions of their places of residence and the obstacles to moving. Although the assessments of experts and professionals are important, it is necessary to understand how older people themselves subjectively appraise the quality of their residential settings. This paper shows how residential normalcy theory portrays the emotion-based experiences of older people and whether they feel their residential or care settings are congruent with their needs and goals, and if not, how they cope with their inadequate environments.
Keywords:aging in place
;
the Residential Normalcy Theory
;
residential comfort emotional experiences
;
residential mastery emotional experiences
;
older Americans
绝大多数(93%)超过65岁的美国老年人居住在普通的住宅和社区,而不是专门规划和建设的养老机构如养老院里。他们大都希望尽可能延长在当前住所居留的时间——即就地养老,拥有自己住房的老年人(占比高达79%)更是如此。约55%的美国老年人在同一个地方居住长达20年以上。有些人即使搬迁,一般也不会搬得太远,通常仍是在同一个州的同一个县境内(U.S. Department of Housing and Urban Development, 2013)。甚至当他们在财务、健康、婚姻状况等方面经历重大变故而不得不开始新的生活方式,或者其居住环境大大改变以后,许多老年人还是希望持续这种就地养老的生活方式。
六组社会学或心理学因素可以帮助解释就地养老对老年人的强烈吸引力(Wiles et al, 2012a; Golant, 2015b)。第一,老年人愿意呆在熟悉的环境中。在这里其对周围事物有更准确、更完整、更可靠的认知,在自己住所和邻里社区周围活动使其感到更有信心、更能应付自如。即使遭遇停电,他们在黑暗中也能在住所内安全地找到所需的东西;同样,他们很清楚社区商店、服务设施及交通路线的具体位置,因此能够以最少的脑力和体力消耗满足自己的日常需要。在熟悉的地方,有朋友跟他们分享愉快的经历,因此不太会感到孤独;并且,当在日常生活中遇到困难需要帮助时(比如想要搭便车去看病或者找人帮忙买东西)时,他们非常清楚该向谁求助。所以,他们会担心,如搬到一个新的社区,需要好几年时间才能重新建立起此类可靠的关系。
第二,老年人对住所内的个人物品怀有强烈的感情。这些看起来仍然有用的东西不仅带给他们快乐,也是家庭财富的一部分,有的甚至可能还值点钱(Ekerdt et al, 2004)。最重要的是,它们是往昔生活的物证,能够唤醒他们对过去的事件、场合及人际关系的记忆,帮助他们回忆生活中曾经的快乐场景和成就(Rubinstein, 1998)。住在旧居里,他们就可以随时凭借这些与过往生活相关的物件去回想这些经历,去回味和享受自己曾经的成功。
第五,许多老年人害怕搬到一个无人认识和了解他们的新社区。他们不想反复告诉别人自己的个人背景和身份以获得认可和接受。他们同时也担心在与别人交流的过程中,谈起自己成功、丰富和有意义的过去时,自己会对生活的价值产生自我怀疑。而在他们居住已久的地方,朋友和邻居们很了解他们,能够欣赏或者至少容忍他们独特的行为或生活方式,他们也无需一直向别人介绍和证明自己(Cumming et al, 1962)。
第六,老年人对自己的隐私十分看重。他们希望自行决定跟谁交往、由谁来探望和看护自己。在自己的住宅或公寓内,他们可以很容易地掌控自己的交往活动;如果搬到其他地方,则难以维持这种自主权。因此,他们不愿搬到某个家庭成员家里或社会性的养老设施内。生活在一个可以控制自己社交活动的地方,对感到自己没有能力抵挡不诚实、不友好、讨厌或暴虐之人的老年人来说尤为重要(Diehl et al, 2003)。
2.2 经济因素
经济因素对老年人就地养老行为的影响比较复杂。例如,并没有可靠证据证明老年人总是搬到生活成本或所得税、消费税、遗产税和房产税更低的地方(Duncombe et al, 2003; Bakija et al, 2004)。如果经济因素是促使他们搬迁的主要动力,则应该有大量的老年人迁往他们成年子女的家里才对,因为在那儿他们可以免交房租。但事实并非如此。即使老年人的房屋开销负担偏重,他们的应对措施通常也不是搬到更便宜的住处,而是减少食物或保健等其他方面的花费、重新找一份工作或者提高信用卡的借贷额度(Pottow, 2011)。
与经济学理论背道而驰的事实是,老年人通常不会把自己的房屋兑换成现金来支付自己的开支,即不愿意消费他们的房产资源。例如,2011年美国仅有7%的65岁以上的老年房主申请房屋净值贷款(equity loans),只有大约2%的老年房主有反向抵押贷款(reverse mortgages,是一种以老年人的房产作为抵押的联邦担保贷款)。相反,他们通常把房产当作支付未来潜在的大笔医疗和长期照护费的资金来源,或想要把房产作为财富转移给子女。老年业主一般不愿意出售自己的房屋,因为担心如果改为租房居住,将面临租金上涨的风险(Masnick et al, 2006)。
身体健康状况变差,使老年人独立生活更加困难。当老年人接近80岁或年龄更高时,罹患各种慢性疾病(如高血压、关节炎、心脏病、癌症、糖尿病、哮喘、支气管炎)的风险会增加。他们将更难料理自身的健康问题,如服药、就医,洗澡、穿衣、吃饭、如厕、修饰、上下床、行走等日常生活活动(activities of daily living, ADLs),以及购物、烹调、做家务、服用药物、处理财务等工具性日常生活活动(instrumental activities of daily living, IADLs)。即使是最基本的室内活动(如爬楼梯、使用壁柜等)也变得很不容易,在光滑的浴室地板上可能会摔倒;无法再开车,这使得他们前往社区商店和其他服务设施变得更加困难。患有老年认知障碍(其中最常见的是阿尔茨海默氏症)的老年人是最需要护理和帮助的群体。他们有情绪和行为障碍、容易四处游荡,需要不间断的监护和协助(Federal Interagency Forum on Aging-Related Statistics, 2012)。
第三,对存在健康问题和活动受到限制的老年人来说,就地养老使他们往往得不到适当的帮助和照顾。家人不一定随时都能提供帮助,收费护工也可能负担不起(Kaye et al, 2010)。而且家人可能并无护理经验或专门训练,偶尔甚至可能出现虐老行为。而私营部门专业人士(如老年科医生、护士、康复专家)供不应求;负责家政和照顾老人的工作人员又常常未经足够培训,或者在夜晚和周末不提供服务(Stone et al, 2010)。
老年人收入水平是决定就地养老质量的重要因素。私营部门提供的照护和服务通常只有经济收入较高的老年人才负担得起,而公共部门提供的价格优惠的服务需要排队等待,并且只有那些收入足够低、没有任何资产的老人才能得到。所以,美国中等收入的老年人最无保障,因为他们既负担不起昂贵的私人保健费用,又没穷到有资格享受大多数公共部门资助项目的程度(Golant, 2015b)。某些特定群体如未婚女性、低收入者以及少数族裔(如非裔和拉丁裔)更是难以得到足够的居家服务和支持,同时生活在偏远郊区和乡村社区的老年人可获得的服务也非常有限(Newcomer et al, 2005)。另一方面,老年人在家中受到太多照顾也未必什么都好。当家庭成员充当照护者时,就会变得更像是职业护工,而不再是情感亲密、地位特殊的家人;辅助设施和医疗设备往往使老年人的住所更像一个养老机构而不是家(Golant, 2015b)。
第四,高龄老年人很有可能独自生活。据统计,2010年美国65岁的老年人中,约19%的男性和37%的女性是独自居住;在七八十岁的老年人中独居比例更高(U.S. Department of Health and Human Services, 2012)。因此,许多老年人受到孤独的折磨。例如,若配偶去世,老年人不仅失去了一个可以依赖的朋友、一个灵魂伴侣,更失去了帮助打理住所或提供交通便利的人。随着时间的推移,重要的朋友去世或者搬迁到其他地方,他们对一幢建筑、一个邻里或社区的眷恋会发生改变。当老年人外出活动能力下降导致无法参加社交活动时,孤独感便会油然而生。他们还会影响到其他老年人的社会行为,因为人们都不愿意经常跟那些比自己更衰弱的人在一起——和他们在一起乐趣不多,而且还时时提醒自己未来也会衰弱不堪。流行病学家发现,孤独的老年人身心不健康的风险更高,因为无人帮助他们应对健康和活动能力下降问题,或者缺乏可信任的人给予情感支持(Greenfield et al, 2011; Perissinotto et al, 2012)。
第五,邻里和社区发生的一些变化会令老年人感到不便。当一家喜欢的商店关闭、一位医生退休,或一条公共汽车线路停止服务,老年人就会感到自己的生活受到困扰。在一些没有活力的老城市、小城镇和农村,失去农业、制造业或能源领域工作的老年人经济上陷入困境。这些社区被称为“老人留守”的地方,因为年轻人口迁移别处寻求就业,留下的是失业的、受教育程度较低的人和老年人(Golant, 1984)。这些地方可能出现社会秩序混乱(如犯罪、毒品、酗酒、破坏公物),建筑物废弃或破败。老年人一般会减少外出,因为独自外出缺乏安全感;并且,这些地方往往缺少休闲娱乐的条件(如公园、广场、图书馆和为老年人组织的活动),及保健和长期照护服务(Krause, 2003; Yao et al, 2008)。
第六,大量的美国老年人住在公共交通不能覆盖的人口稀疏的城市郊区或农村地区。当他们还能开车时,购物等日常活动尚无多大困难。然而随着年龄增大,开车变得不可能或不安全。许多上年纪的寡居老人也存在交通困难,因为她们再也不能依靠丈夫送自己到目的地(Mezuk et al, 2008; Connell et al, 2013)。出行不便的老人不仅更少参加休闲或社交活动,而且会减少购物和看病的次数(Baily, 2004)。一些老人搭便车或使用叫车服务,但如此一来他们就失去了自行或预先安排行程的自主性;在晚上或周末他们需要外出时更是困难重重。
3.2 缺少其他可行的选择
对老年人可能经历的上述问题的分析表明,相关政策的制定者和实施者必须清楚,即有些老年人就地养老并不是因为他们觉得住在家里有多好,而是因为他们没有更好的选择,只好“被困在家里”(Torres-Gil et al, 2012)。研究表明,在以下情况出现时老年人才会自愿决定搬迁(Golant, 2011)。
第四,对搬迁行动不感到过度紧张。不管现住所的问题有多严重,新居处安排有多理想,一些老年人还是会认为搬迁过程本身太累人、累心或费钱。例如,老年人可能不希望花费必要的精力去寻找新居住地或搬动物品。并且,老年人对自己存活期的预判可能会影响他们对这些代价是否值得的评价;如果他们觉得自己只能活不多的几年,就不情愿承担这些麻烦,因为他们认为这样做得不偿失(Carstensen et al, 1999)。
因此,居住常态理论认为,当老年人感觉自己处于居住舒适区或掌控区之外时,会使用人类发展理论家称之为适应(accommodative)或同化(assimilative)的应对策略(Brandtstädter et al, 1994)。正如Golant(2015a)所说:“适应反应是指思维策略,老年人通过降低对环境的预期或愿望,从心理上淡化其住所缺点的影响,说服自己这些不完全合适的居住条件对他们的自尊心、自我认同或幸福感并没有那么重要。同化反应是指行动策略,即老年人改变他们对住宅环境的居住或使用方式,来改变其不适宜的设施或功能”。
按照居住常态模型理论,老年人需要开展第二次评估过程(Lazarus et al, 1984)以决定如何消除或缓解居住地的不适宜性(Golant, 2015a)。这些评估使一些老年人比其他人采取了更成功的适应策略。该模型认为这些老年人具有更丰富的应对办法。也就是说,他们对什么是有效的应对策略有更清楚的认识,这使得他们能够及时、有效地处理问题(不管这些问题有多复杂),获得可行的解决方案。有效应对措施的标准是既不会使身、心和财力上产生负担,也不能与他们的生活方式相冲突,或强迫他们违背自己的价值观和信仰。采取这些应对策略产生的间接成本较低。
(1) 他们是更具灵活性的个体(Skodol, 2010; Aldwin et al, 2012; Wiles et al, 2012b; Wild et al, 2013)。他们具有的个性、价值观和人口统计学特征(年龄、职业、文化、收入等)激励和帮助其找到创造性和建设性的自我适应策略来应对逆境。例如,他们可能有更丰富的技巧去解决问题,或丰厚财力使其更容易承担额外成本。这些老年人过去的生活经历使其更有能力解决遇到的问题。他们可能具有信任他人和开放的个性,容易得到别人帮助和支持,因此会积极寻求解决问题的方案。他们也可能是更快乐的人,对生活具有乐观的看法,从而对自己的未来更有希望。
(2) 具有丰富应对技能的老年人多居住在或可以搬到更具弹性的社区。这些社区很好地适应了帮助其老年居民应对挑战的过程,为居民提供了更多的机会和资源来实现其居住常态(Hall et al, 2010)。在这些地方,老年人可以得到更多有趣或愉快的经历(如更多的朋友、有吸引力的休闲机会,或更少的住宅维修等的麻烦)。这些地方提供了适合老年人生活方式和使用需求,价格实惠或设计精良的住宅或建筑物。此外,这些地方为身体衰弱的老年人提供更多的长期支持和服务,使他们能够应付自己的局限性和慢性健康问题,进而帮助其提升自我评价(感觉自己更有能力、更自主和更有控制力)。这些社区有(来自公共、私有和非营利部门)思维更超前的领袖,能够认识到通过改善其财务资源、教育或培训、公民参与状况以及组织和解决问题的能力,从而帮助老年人的重要性。
(3) 有丰富应对技能的老年人通常自主决定居住和护理事务或自愿将这些决策责任转交给他们信任的人。对经历身体衰退和认知下降的老年人来说,能自主选择自己的应对方案显得更加具有挑战性。在此情况下,成年子女或聘请的专业人士经常试图强迫老年人接受他们的居住和保健选择。然而,有证据表明,当老年人对自己的决策失去控制,或对自己居住和医疗事务的决策人的动机不信任时,其对生活质量的体验将更为负面(Langer et al, 1983; Lieberman, 1991; Morgan et al, 2013)。
The majority of older Americans in their mid-60s and older(93%) occupy ordinary dwellings and community settings as opposed to purposively planned and developed residential care facilities, such as assisted living developments or nursing homes. They also strongly prefer to remain as longtime residents in their current dwellings, that is, to age in place, especially the 79% who are homeowners. About 55% of the U.S. older population has lived at the same address for 20 or more years. Moreover, even when they do move, their new addresses are usually a short distance away, often within the same counties of their states(U.S. Department of Housing and Urban Development, 2013). These residential inertia patterns often persist even after older people experience significant changes in their financial, health, and marital status, embark on new lifestyles, or their residential environments substantially change.
This paper reviews the strong attractions of their current residences to explain the aging in place behaviors of older people, although the paucity of available and viable housing alternatives also explains their residential inertia. This overview also emphasizes that the residential arrangements of older people are often more than just places to live. When older people confront difficulties living independently, they often modify their dwellings to make it easier for them to cope with their chronic health problems and physical and cognitive limitations. Consequently, they might add grab-bars in their bathrooms, install raised toilet seats, add handrails to their staircases, or install an emergency response system to alert others when they fall. Their homes will also be frequented by both informal(e.g., family members) and formal(paid professionals or home care workers) caregivers who offer them a variety of health, rehabilitative, and supportive services. Because of these physical modifications and the provision of in-home assistance, the residences of older Americans have often become de facto care settings(Golant, 2015b). Consequently, when we study the quality of life of older Americans, we often must recognize that they are sometimes living in both residential and care environments.
When scholars judge the suitability of the residential and care environments occupied by older people, their conclusions will depend much on their worldviews. On the one hand, they can base their findings on the expert judgments of academics and professionals; on the other hand, they can rely more heavily on how older people feel about their residential worlds. In recognition of the importance of this second worldview, this paper outlines an emotion-based theoretical model that shows how the subjective environmental experiences of older people influence their aging in place or moving decisions. This model also argues that when older people find themselves in incongruent residential settings, they usually initiate adaptive or coping strategies that can alleviate their adverse circumstances.
2 Explaining the aging in place behaviors of older Americans
2.1 Social and psychological factors
Six sets of social or psychological factors help explain older people's strong attractions to their current places of residence(Wiles et al, 2012a, Golant, 2015b). First, older people want to remain in familiar environments. Here they have more accurate, complete, and reliable cognitive maps of their surroundings. Consequently, they feel more confident and competent navigating around their dwellings, neighborhoods, and communities. If they lose electrical power, even in the dark they can safely find things in their dwellings. Similarly, they have good knowledge of where the stores, services, and transportation routes are in their communities and can satisfy their everyday needs with minimal mental and physical energy. In their familiar places, they have friends to share enjoyable social experiences and thus are less likely to feel alone. They are also more aware of who they can count on when they need assistance with their everyday needs—whether getting a ride to their doctors or assistance with their shopping. These older people reason that it would take years for them to establish such reliable connections in a new community.
Second, older people have strong emotional attachments to the personal belongings in their dwellings. These possessions give them pleasure, still seem useful, are part of a family's legacy, and perhaps are even worth money(Ekerdt et al, 2004). Perhaps more importantly, they constitute archeological evidence or material signposts of their pasts that enable them to recall memories of events, occasions, and relationships. Thus, these possessions become catalysts for their reminiscing(or life reviews) helping them to recall the happy occasions in their lives and their successful achievements or accomplishments(Rubinstein, 1998). Moreover, they can choose when to recall these experiences and enjoy their pasts. They control this activity.
Third, older people are often proud of their current dwellings, neighborhoods, or communities. Consequently, their built or material settings offer evidence to their friends and families that they are accomplished individuals who have lived successful lives. The opinions of others may be especially important to older widows who owe their current socioeconomic status and material possessions to the accomplishments of their now deceased husbands. These older women fear that if they vacate their current houses, they would abandon their only material evidence that they had competent and worthy lives(Kemper, 1978).
Fourth, many older persons stay put because they are averse to experiencing novel events and activities. They enjoy the sameness or continuity of their activities, events, and environments. They fear that in a new place of residence they would continually have surprising, unsettling, and unpredictable experiences(Klapp, 1986). Rather, they favor remaining in places where they can enjoy their ritualistic activities of everyday living—whether watching their TV programs in their favorite rooms, walking their dogs, participating in Sunday church services, or meeting at a familiar restaurant with good friends.
Fifth, many older people dread the prospect of moving to a new community where nobody knows anything about their lives. They do not want to re-educate others about their personal backgrounds and identities as a way to gain recognition and acceptance. They worry too that in the process of communicating to others about their successful, productive, and meaningful pasts, they will begin to have their own self-doubts about the worthiness of their lives. Such conversations are unnecessary where they now live, because their friends and associates know them very well, appreciate or at least tolerate their distinctive behaviors or lifestyles, and they do not have to continually impress these significant others about their loyalties(Cumming et al, 1962).
Sixth, older people value highly their privacy. They want to decide with whom to communicate and who watches and monitors them. They fear that if they move elsewhere, they will have more difficulty maintaining this territorial control. They especially want to control their interpersonal interactions when in their dwellings or apartment buildings. These privacy concerns help explain their reluctance to relocate to the home of a family member or to a group residential facility, such as an assisted living development. Living in a place where they can control their social interactions are especially important for physically vulnerable older persons who feel less able to fend off dishonest, unfriendly, irritating, or abusive people(Diehl et al, 2003).
2.2 Economic factors
Economic factors also contribute to the aging in place behaviors of older people but not in straightforward ways. There is no compelling evidence, for example, that older people always relocate to places with a lower cost of living or lower state income and sales taxes, inheritance and estate taxes(Duncombe et al, 2003; Bakija et al, 2004). If economic factors primarily motivated their moves, much larger numbers of older people would be relocating to the homes of their adult children where they could live rent-free.
Even when older people occupy dwellings with burdensome housing expenses, they often cope not by moving to less expensive accommodations, but by cutting back on what they spend on other items(e.g., food or health care), by returning to work, or alternatively by increasing their credit card debt(Pottow, 2011).
Contrary to economic theory, older people are usually reluctant to use(cash out) their dwellings' equity(home value less mortgage loan debt) to help pay for their housing expenses—that is, consume their housing wealth. In 2011, for example, only 7% of homeowners age 65 and older had home equity loans, and only about 2% had reverse mortgages(federally insured loans that enable older people to receive a substantial amount of their home's equity in the form of cash advances). Rather, older people usually treat the equity in their dwellings as a "rainy day" funding source to cover their potentially large future medical and long-term care expenses or as a way to transfer their wealth to their children. Older homeowners also fear that if they become renters, they will risk having continual and unexpected rent increases(Masnick et al, 2006).
Some economic factors underlying their aging in place are unique to particular historical periods. During the 1990s and early 2000s, house prices in the United States increased substantially. Consequently, some older people sold their dwellings, moved to less expensive housing, and realized significant cash returns. However, many other older people were reluctant to sell in such an appreciating housing market because they feared that if they sold too early, they would not realize even higher housing prices. Moreover, if they decided to downsize and move to smaller dwellings, they worried about paying inflated prices for their new residences.
Subsequently, the great economic recession in the United States between 2007 and 2010 also produced some uniquely powerful aging in place influences. Over this period, housing values in most places declined sharply. Consequently, older people who might have seriously contemplated moving postponed these residential transitions because they were reluctant to realize equity returns far below their expectations. Additionally, because of the depressed economy and the unavailability of mortgage financing, there were few buyers for their homes. The stock market declines, smaller private pension benefits, and lower interest rate and dividend returns on their investment portfolios and savings accounts also increased the income insecurity of older people. Consequently, over this period, smaller shares of older people retired, but as a result they were restricted to residences near their job locations, a powerful moving constraint(Golant, 2008a).
2.3 Declines in physical health and greater difficulties living independently
When older people reach their late 70s and older, they are at increased risk of having various chronic health conditions(e.g., hypertension, arthritis, heart disease, cancer, diabetes, asthma, bronchitis). They have more difficulty managing their health problems—taking their medications and getting to their doctors; performing self-care tasks or activities of daily living(ADLs) such as bathing, dressing, eating, using the toilet, grooming, getting in or out of bed, or walking; and performing instrumental activities of daily living(IADLs), such as shopping, preparing meals, doing housework, taking medications, and handling their financial affairs. Even the most taken-for-granted activities in their dwellings become difficult, such as climbing stairs or reaching their closet shelves. They worry about falling on the slippery floors of their bathrooms. They have to stop driving which makes it more difficult for them to reach the stores and services in their communities.
Older persons who suffer from dementia, the most common being Alzheimer's disease, have some of the most demanding care and assistance needs. They require continual supervision and queuing to do everything, experience mood and behavioral disorders, and are prone to wandering(Federal Interagency Forum on Aging-Related Statistics, 2012).
Confronted with these physical and mental declines, we might expect that older people would move to group residential care facilities(e.g., assisted living) or to the home of a family member to obtain more assistance. However, this is usually not the case. Rather, older people cope with their aging bodies by modifying their current dwellings, such as by adding grab bars, installing nonslip floors, or improving their dwelling's lighting. Alternatively, they make few adjustments to their accommodations and simply avoid the offensive aspects of their residences—for example, they live on the first floor of their two-story houses. When physical modifications are insufficient, they solicit the help from family members; or they take advantage of the home- and community-based services available in their community, some targeting low income older people(National Consumer Voice for Quality Long-Term Care, 2012, Golant, 2015b).
2.4 Societal and groupthink factors
Older Americans hear a repetitive message from the print and internet media, experts in aging, long-term care providers, and family members who claim to know what is best for them. This "groupthink mindset" cajoles older people not to move but to cope with their health problems and impairments in their familiar dwellings. It considers any other solutions to be inferior, uninformed, or ill advised. The groupthink mindset argues that aging in place is the only right way to live out one's life(Golant, 2008a, 2009).
This messaging is also occurring at a time when older people in the United States have many private and public sector options to help them to age in place. They can physically modify their dwellings to make them more congruent with their aging bodies, obtain assistive devices(e.g., canes and walkers), install medical monitoring and home security technologies in their dwellings, and obtain personal assistance and care from an historically high number of home care providers(Golant, 2015b). So-called age-friendly buildings, neighborhoods, and communities offer older people a variety of volunteer-provided and price discounted services that make it easier for them to age in place(Golant, 2014). Numerous federal and state public policies target lower income older people and offer them property tax relief, home repair and modification solutions, and affordable home care assistance. However, as I emphasize below, these societal responses are often far from perfect solutions and are not available to all segments of America's old.
3 Housing problems confronting older people in the united states
3.1 Six different categories of housing and long-term care problems
Despite their reluctance to move, a significant share of older people in the United States suffer from as many as six different categories of housing and long-term care problems.
First, older people are sometimes overburdened by their housing costs, which constitute 35% of their household expenditures, and 43% of the expenditures of those in the lowest income quartile(Social Security Administration, 2013).These costs primarily include the rent and utilities of renters and the mortgage payments, property taxes, and property insurance of owners. In 2011, 61% of renters and 35% of homeowners age 65 and older paid more than 30% of their household incomes on these housing expenses. About 36% of renters and 18% of owners paid monthly dwelling costs that were more than 50% of their incomes(U.S. Department of Housing and Urban Development, 2013).
Some groups of older people have especially high dwelling expense burdens and include the poor, African Americans and Hispanics, unmarried women, and the less educated. Lower income older homeowners still paying off their mortgages are especially burdened(AARP Public Policy Institute, 2011). Older people in the United States today are much more likely to be still paying off their home loans than in the past. In 2010, this included 54% of age 55~64, 41% of age 65~74, and 24% of age 75 plus homeowners(Trawinski, 2012).
A second set of problems result from older people occupying older housing. In 2011, more than a third of their dwellings were at least 50 years old(Golant, 2008b). As I summarized elsewhere: "Older buildings are especially at risk of having three categories of physical deficiencies: physical disrepair requiring equipment or infrastructure upgrades; outmoded physical design features; and physical features incompatible with the mobility or sensory declines of their occupants"(Golant, 2015b). These deficiencies influence the lives of older people in several ways:
· They are at greater risk of experiencing expensive dwelling repair bills(e.g., breakdowns in their air conditioning or heating), which if left unattended may jeopardize their physical health.
· They are more exposed to environmental hazards, such as dust, mold, dampness, lead, air pollutants, and bacterial infections.
· They are more susceptible to invasions from termites, rodents, roaches and other pests, which also expose them to threats such as toxins, vermin, and allergens.
· Their houses are less energy-efficient, which means higher monthly bills for heating and cooling.
· Their houses usually have out-of-date room layouts, flooring, lighting, closet space, décor, are uncomfortably large, and thus may be incompatible with their retirement lifestyles.
· Their dwellings often have rooms and bathrooms only accessible by walking up stairs or they have hard to reach shelves and cupboards.
· They have slippery bathroom and shower area floors, and slick kitchen linoleum floors, that increase their risks of falling(Golant, 2008b).
Third, when older people with health problems and mobility limitations opt to age in place in their current dwellings, they often do not get sufficient or good quality assistance and care. Some older people cannot always count on help from their family members or alternatively afford the care offered by paid workers(Kaye et al, 2010). Even when family members are available, they may have little care experience or training, and sometimes may even be guilty of abusive behavior. Private sector professionals(e.g., geriatric doctors, nurses, rehab specialists) are often in short supply; and hands-on(direct care) workers assisting with homemaking and self-care tasks often have insufficient training or are unavailable when needed—e.g., nights and weekends(Stone et al, 2010).
The incomes of older people matter. The care and services offered by the private sector are usually only affordable to higher income older people; and public sector solutions—which often have waiting lists—are only available for those with sufficiently low incomes and few assets. Perhaps surprisingly, middle-income older people in the United States often have the most difficulty securing assistance because they cannot afford the high costs of private care, yet they are not poor enough to be eligible for most public sector sponsored programs(Golant, 2014a, Golant, 2015b). Certain older groups are more at risk of not receiving adequate long-term services and supports in their homes: unmarried women, those with lower incomes; and minority groups, such as African Americans and Hispanics. Older persons living in more service-deficient and isolated locations—in outlying suburban and rural communities—also have more limited service options(Newcomer et al, 2005).
Paradoxically, there are also downsides if older people receive too much care in their homes. When family members serve as their caregivers, they often act more like professional workers than emotionally close significant others; and the introduction of assistive devices and medical equipment often makes the dwellings of older people look and operate more like an institution(e.g., a nursing home) than a residential setting(Golant, 2015b).
Fourth, at higher chronological ages, people are more likely to live alone. In 2010, about 19% of men and 37% of women age 65 and older lived alone and these percentages are higher for those in their 70s and 80s(U.S. Department of Health and Human Services, 2012). Consequently, many older people feel lonely and isolated. With the death of a spouse, for example, the older person can no longer count on a trusted confidant, a soul mate, or more practically, someone who had helped them maintain their dwelling or provided transportation. Over time, the social desirability of a building, neighborhood, or community changes after valued friends die or move away to other locations. Loneliness is also a consequence of older people experiencing mobility declines that prevent them from participating in social activities. Sadly, these declines also influence the social behaviors of other older persons. They often are reluctant to engage in activities with those who they perceive as more vulnerable than themselves, because they are no longer fun to be with or because they remind them of their own vulnerable futures.
Epidemiologists report that older people who are lonely are at greater risk of experiencing other adverse physical and mental health outcomes because they lack persons to help them cope with their health problems or mobility declines or because they lack the emotional supports of trusted individuals(Greenfield et al, 2011; Perissinotto et al, 2012).
Fifth, older people find themselves in neighborhoods and communities that have experienced undesirable physical or demographic changes. The lives of older people are disrupted when a favorite store closes, a doctor retires, or a bus service stops. Other communities—in older cities, small towns, and rural counties—decline economically because they have lost jobs in their agricultural, manufacturing, or energy sectors. Sometimes they are referred to as "aged left behind" localities, because younger populations migrate elsewhere seeking jobs and the unemployed, less educated, and older populations are left behind(Golant, 1984) . These places are more likely to have social disorders, such as crime, drug and alcohol use, and vandalism and have abandoned or physically rundown buildings. Older people in these locales tend to venture out less frequently, feel insecure walking alone, and they lack the supports of trusted neighbors. These places often lack recreational amenities(e.g., parks, public squares, libraries, and organized events for older people), but also healthcare and long-term care offerings(Krause, 2003; Yao et al, 2008).
Sixth, large shares of older people in the United States occupy low-density cul-de-sac urban suburbs or population sparse rural areas where public transit is unavailable. When these residents could drive, they had little difficulty reaching their everyday goods and services. However, when they experience the physical or cognitive declines of aging, driving becomes impossible or unsafe. Many older widows also experience transportation difficulties because they can no longer rely on their husbands to drive them to their destinations(Mezuk et al, 2008; Connell et al, 2013). Lacking reliable transportation, older people not only engage in fewer recreational or social activities, but also curtail their visits to their grocery stores and doctors(Baily, 2004).
Some older people are able to compensate by sharing auto rides with others but then their activities become dependent on the schedules of others. Others benefit from demand-responsive(or paratransit) alternatives that pick them up at their homes and deliver them right to their destinations. However, this mode of transportation is also not without downsides because older persons must be willing to arrange all their trips ahead of time and these services are not always available during evenings or weekends.
3.2 An absence of alternatives
When older people experience these problems, practitioners and policymakers must be alert to the possibility that they are aging in place not because of the attractive features of their residences, but because they feel "stuck in place" and have no viable moving options(Torres-Gil et al, 2012). Older people typically decide to move—at least voluntarily—only if they have satisfied the following five conditions(Golant, 2011).
First, older people contemplate moving only when they have exhausted their efforts to resolve their current incongruent housing situations. For example, they cannot find enjoyable leisure activities in their community; they cannot find extra funds or part-time work to pay for their burdensome dwelling costs; they have trouble finding new friends to lessen their loneliness; or they have no family to ask for assistance with their self-care needs.
Second, older people must believe that moving to another place is a credible option. They must be aware of alternative places to live that fit their lifestyles, help them deal with their limitations, and are affordable. If homeowners, they must be able to sell their dwellings at an acceptable price. They must also be willing to cope with the potentially disruptive changes, however, positive that they are likely to experience in a new community.
Third, there must be a synergistic relationship between the factors that are "pushing" older people from their current residences and "pulling" them to an alternate destination. It is unrealistic to speak of push and pull moving factors as if they are independent forces. The positive attractions of a new housing situation must outweigh the negative aspects of where older people now live. Moving must produce a net gain of housing benefits.
Fourth, however, serious their current housing problems or desirable their alternative residential arrangements, older people must not appraise the act of moving as overly stressful. Some older people will evaluate the moving process itself as too physically exhausting, psychologically demanding, or financially expensive. For example, older people may not want to spend the necessary energy searching for a new place of residence or to move their possessions. How close older people perceive their own death may influence how they evaluate these costs. If they feel they have only a few years left to live, they will be less willing to incur these costs because they will have only a relatively short time at a new destination to enjoy the compensating benefits(Carstensen et al, 1999).
Fifth, other persons in the household or influential family members must be supportive of the moving decisions of older persons. This may be difficult for two reasons. First, when older persons are married, both spouses must reach consensus on the moving decision. But this may be difficult when the two individuals have very different retirement goals, are at very different stages of their work careers(e.g., one still working, the other retired), or have different unmet long-term care needs. Second, when older people experience physical or cognitive declines in their health and functioning, they may have less say about where they move because family members or professionals have a greater decision-making influence.
4 The residential normalcy theoretical model
Academics and professionals often judge the quality of older people's housing by relying on their detached scientific or objective indicators. But older people do not always agree with these appraisals. Their considerations of the pros and cons of where they live depend on how they personally interpret and evaluate these indicators. A variety of individual attributes that have distinguished older people throughout their lives will influence these subjective assessments, including their personalities and demographics. Older people will also differently evaluate their current housing situations because of their past residential experiences. And their appraisals will depend also on whether they have incurred declines in their health and difficulties performing their ADLs and IADLs(Golant, 1998).
To understand how older people judge their places of residence, this paper presents an overview of an earlier constructed residential normalcy theoretical model(Golant, 2011). It proposed that older people will occupy congruent residential settings that are consistent with their needs and goals when they report overall favorable or positive emotional experiences.
It further explains why some older people cope more effectively when they experience problems or inadequacies in their places of residence(Fig.1).
Geographers have long recognized the importance of studying how people feel about the places where they live and conduct their activities(Rowles, 1978; Milligan, 2005; Andrews et al, 2013, 2014; Skinner et al, 2015). Similarly, psychologists have argued that the emotional reactions of individuals represent "the common core of human response to all types of environments”(Mehrabian, 1980). Life-span scholars have particularly recognized the motivational roles played by emotion as(Magai, 2001) emphasizes:
"They [are] integral to our sense of well-being or lack of well-being…They are what make individuals care about outcomes, and care in particular ways, with fear, revulsion, joy, shame, excitement, guilt, indignation, and so forth."
The proposed theoretical model distinguishes two independent categories of emotional experiences: residential comfort and residential mastery emotional experiences. The model theorizes that older people achieve residential normalcy when they occupy places in which both sets of these experiences are overall favorable or positive(Golant, 2011).
4.1.1 Residential comfort experiences
The first category, residential comfort experiences, captures the extent to which older people feel that their dwellings and their neighborhood and community environs are pleasurable, comfortable, and enjoyable places to live. When these experiences are positive, older people variously feel contented(vs. discontented), stimulated(vs. bored), cheerful(vs. glum), accepted(vs. rejected), and delighted(vs. disgusted). This category also captures whether older people are experiencing the hassles of life, "the irritating, frustrating, distressing demands that to some degree characterize everyday transactions with the environment"(Kanner et al, 1981). Examples include, shoveling snow, interacting with an annoying neighbor or an irritating staff person. Some experiences in this category are not a result of current environmental transactions, but rather are a product of past activities and events. These residential memories also constitute an important source of their pleasurable(or unpleasurable) experiences.
Older people may not agree on what constitute the pleasurable or enjoyable aspects of their places of residence(Golant, 2015b):
· For some, it will be places with a warm year-round climate; for others it will be where the seasons change.
· A large and diverse city with lots of restaurants, shops, theaters, and street activity will be appealing to some; others will be happiest in less bustling and quieter rural settings where they are close to nature.
· Some will be content spending their days in their gardens, playing cards, reading books, listening to music, and having quiet gatherings with a few close friends; others will be most uplifted when they spend time outside their dwellings and they are actively involved in their communities participating in religious activities and volunteering(civically engaged) for important causes.
· Some will enjoy places where they continually have new experiences; others will enjoy residential situations that allow them to pursue familiar social and recreational activities.
· Some will feel that they are inseparable from the treasured stuff that they have collected over their lives; others will dispose of it as junk.
· Some will enjoy being alone; others will feel happiest when they are mingling with family and friends.
· Some will enjoy living in active adult communities specifically offering recreational opportunities for older people; others will be depressed living with people only their own age.
4.1.2 Residential mastery experiences
The second category, residential mastery experiences, captures the extent to which older people occupy residential or care settings in which they feel competent and in control. When older people have such favorable experiences, they variously feel influential (vs. influenced), dominant(vs. submissive), autonomous(vs. dependent), secure(vs. anxious), powerful(vs. overpowered), strong(vs. helpless), encouraged vs.(frustrated), confident(vs. uncertain), and unafraid(vs. afraid). Four sets of interactions that older people have with their environments will increase the likelihood that they feel incompetent.
First, older people experiencing health problems and mobility limitations feel more vulnerable when they confront difficulties or constraints when using or accessing their residential settings. They feel less capable when their stairs are difficult to climb, faucets more difficult to turn, and high closet shelves difficult to reach. When their neighborhoods lack sidewalks, are not well designed or maintained poorly, and when their streets are difficult to cross because of traffic conditions, older people will feel less secure or more afraid to walk outdoors. When they occupy physically remote rural locations, they feel less able to reach even their most necessary destinations, such as food or medical assistance, or to spend time with friends or neighbors.
Second, when older people suffer personal losses, such as the death of a spouse or a close friend, they not only lose enjoyable and pleasurable relationships. Additionally, because these significant others had physically assisted them with their everyday tasks, whether housework or getting to places, their absence now reminds them of their mobility shortcomings. They also lose persons who made them feel useful and reminded them of their successful and productive lives.
Third, older people will have heightened feelings of incompetence when they experience declines in their cognitive and sensory skills. Driving a car becomes more problematic because they take longer to reach their destinations, get lost more often, and are afraid to drive at night. Ultimately, they must give up their car keys and suffer declines in their transportation mobility and feelings of efficacy.
Fourth, older people often feel more incompetent when they no longer feel proud of where they live. These persons are upset that their dwellings do not communicate to valued friends or family members that they have had successful, worthy, or accomplished lives. Consequently, they begin to have doubts about the value of their lives. These feelings are especially palpable when these older persons no longer garner the respect they once had as productive members of the workforce or as valued members in their community.
Second, older persons feel less in control when their privacy is threatened. This occurs when they cannot influence who sees, hears, and talks to them, and who monitors—administratively or technologically their activities, behaviors, and movements. These are often the feelings expressed by older people who are dependent on their family members for assistance. Consequently, they find it difficult to avoid their intrusions and choose when to be alone.
Third, they feel insecure when they must deal with persons who they no longer trust—whether friends, family, staff, or professionals. They are no longer confident or feel certain that these persons will be responsive to their needs and goals, keep their promises, and respect their preferences.
Fourth, older persons no longer feel in control over their lives, when they lose the ability to manage their own financial affairs(e.g., paying their bills; managing their investments), tasks they were responsible for most of their adult lives.
4.2 Congruent residential settings
The residential normalcy theory assumes that older people are able to sort through each of their sets of residential comfort and residential mastery experiences and judge them as positive or negative. It also assumes that they can differentiate their experiences according to their salience, that is, how much or to what extent they satisfy(or do not satisfy) their most important residential needs and goals. For example, older people might judge a neighborhood’s physical appearance and the nearness of a family member as equally positive experiences. However, being close to family may be crucial for helping them maintain their independent households, whereas the quality of their neighborhood plays a very small role in their current lives.
In the best case scenario, older people will be in their residential comfort zones when they get pleasure or enjoyment from their places of residence, do not feel hassled, and have good memories of their residential pasts; and they will be in their residential mastery zones when they feel competent and in control of their residential surroundings. When older persons are both in their residential comfort and residential mastery zones, they have achieved “residential normalcy.” These are places(Golant, 2011):
"Where older people experience overall pleasurable, hassle-free, and memorable feelings that have relevance to them; and where they feel both competent and in control—that is, they do not have to behave in personally objectionable ways or to unduly surrender mastery of their lives or environments to others."
In the worst case scenarios, older people will occupy altogether incongruent residential or care settings and be out of both their residential comfort and residential mastery zones.
However, the theorized orthogonality or independence of the residential comfort and residential mastery sets of emotional experiences introduces the possibility that congruence may not be an all or nothing affair. That is, it is possible for older people to occupy places that offer features and activities that make them appropriate places to live, but at the same time have highly undesirable qualities. In the language of the model, older people may find themselves in their residential comfort zones, but out of their residential mastery zones, or vice versa(Fig.2). For example, they may enjoy living in their current place of residence because of good friends, attachments to their possessions, good climate and few hassles(that is, they feel in their comfort zones); however, their health problems and walking limitations may make it difficult for them to get their groceries, maintain their dwellings, or manage their medications without help(that is, they feel out of their mastery zones). On the one hand, older occupants of an assisted living development (facility that offers care to frail older people) may feel secure because they have their everyday needs taken care of (that is, they feel in their mastery zones). On the other hand, they feel it is an unpleasant place to live because their apartments are too small and the other residents are unfriendly (that is, they feel out of their comfort zones).
4.3 Coping with adversity or incongruent residential or care environments
Studies assessing whether older people occupy congruent residential settings are typically point-in-time or cross-sectional analyses. Consequently, most researchers of the housing conditions of older Americans prematurely end their analyses after they find that their sample of respondents occupy poor quality residential environments. The residential normalcy theory argues that this static perspective is unrealistic(Golant, 2015a). At various times over their lifetimes, older people may find themselves in residential situations that are inconsistent with their lifestyles or capabilities. However, this is not their end game. Human development theorists tell us that successfully aging older people do not give up attempting to find appropriate places to live and that their environmental incongruence may be a momentary occurrence. Rather, they proactively initiate coping behaviors—that is, they actively seek solutions to eliminate or alleviate their housing problems.
Consequently, the residential normalcy theory argues that when older people feel out of their residential comfort or residential mastery zones, they initiate what human development theorists identify as accommodative or assimilative forms of coping(Brandtstädter et al, 1994). As summarized elsewhere(Golant, 2015a):
"Accommodative adaptive responses(or secondary control) refer to mind strategies whereby older persons deal with their negative appraisals by lowering their environmental expectations or aspirations, de-emphasizing their salience, or variously rationalizing that their incongruent residential arrangements are not that important for their self-esteem, self-identity, or happiness."
"Assimilative(or primary control) adaptive responses, on the other hand, refer to action strategies, whereby older persons change how they occupy or use their residential environments and eliminate or change their incompatible content or features."
Theorists usually equate aging successfully with older people initiating assimilative coping actions, whereas they initiate accommodative adaptations when they feel overwhelmed and hopeless because of the severity of their problems. Older persons seeking to achieve residential normalcy can initiate two very different categories of assimilative responses. First, they can decide to stay put in their current residential settings and cope with their negative experiences by modifying, avoiding, or compensating for their incongruent environmental aspects. For example, to feel again in their residential comfort zones they find more enjoyable leisure or recreational activities or new friendships in their communities; or to feel again in their residential mastery zones, they hire a live-in helper to help them perform or manage their health problems and self-care tasks. Second, they can cope with their unsatisfactory residential arrangements by moving elsewhere—to a new dwelling or community(Fig.3).
Fig.3 Alternative strategies to cope successfully when out of residential mastery zone
Importantly, when older people successfully cope with their difficulties, they do not necessarily "bounce back" to some original starting point or equilibrium(Davoudi, 2012). Consequently, when they again occupy places congruent with their needs and goals and have achieved residential normalcy, their new environments may have very different qualities and they may be conducting different activities or practicing different lifestyles. Consequently, older people may experience several new residential normals over their lives. As I emphasized earlier(Golant, 2015a):
"[Older people] do not necessarily replace lost activities, re-establish the integrity of a past residential setting, or maintain the continuity of their past lives or environments. They end up in residential or care settings and conducting activities different from their pasts."
4.4 Why do some aging in place older people cope more successfully with their problems?
The residential normalcy model theorizes that older people must engage in a secondary appraisal process(Lazarus et al, 1984) to decide on how they might eliminate or alleviate their incongruent places of residence(Golant, 2015a). However, these deliberations result in some older people initiating more successful adaptive strategies. The model argues that these persons have more enriched coping repertoires. That is, they will be more aware of coping strategies that they appraise as efficacious, enabling them to timely manage or successfully resolve their problems whatever their complexity; and these will be more viable or doable solutions. That is, older people will appraise these coping efforts as less physically burdensome, strenuous, financially overwhelming, or less likely to clash with their lifestyles or force them to violate their values or beliefs. To initiate these coping strategies, older people will incur lower collateral costs.
The theory proposes three factors to explain why some older people have more enriched coping repertories(Fig.4). First, they will be more resilient individuals(Skodol, 2010; Aldwin et al, 2012; Wiles et al, 2012b; Wild et al, 2013). They will have personalities, values, and demographics that motivate and enable them to find creative and constructive adaptive strategies to deal with their adversity. For example, they may have stronger problem-solving skills or have financial resources that make it easier for them to tolerate the collateral costs connected with implementing their coping solutions. The past life experiences of these older individuals will have better prepared them to deal with their problems. They are likely to have personalities predisposing them to finding solutions because they are more trusting and open to receiving the help or supports of others. They are also likely to be happier persons who have optimistic outlooks on their lives and are therefore more hopeful about their futures.
Fig.4 Factors influencing secondary appraisals of coping repertoires by older adults
Second, older persons with enriched coping repertoires will occupy or can move to more resilient communities that have better adapted to the challenges faced by their older residents. These communities offer their residents more opportunities or resources for them to achieve their residential normalcy(Hall et al, 2010). In these locales, older people find more enjoyable or pleasurable place experiences(e.g., more friends, attractive recreational opportunities, or fewer dwelling maintenance hassles). These places offer more affordable or better designed dwellings or buildings that cater to the lifestyles and accessibility needs of older adults. Additionally, these places offer their physically vulnerable older occupants more long-term supports and services that enable them to cope with their limitations and chronic health problems and thus help them feel more competent, autonomous, and in control. These communities will have more forward thinking leaders(from the public, private, and nonprofit sectors) who recognize the importance of empowering older persons by improving their financial resources, education or training, civic engagement, and organizational and problem-solving skills.
And third, older people with more enriched coping repertoires typically make their own residential and care decisions, or have voluntarily shifted these decision-making responsibilities to persons they trust. Being able to select their own coping options becomes more challenging for older people who have experienced physical and cognitive declines. In these instances, their adult children or hired professionals often try to compel them to accept their residential and care choices. However, evidence shows that when older people lose control over their decision-making or do not trust the motives of those making their housing and care decisions, they experience more negative quality of life outcomes(Langer et al, 1983; Lieberman, 1991; Morgan et al, 2013).
5 Postscript
Looking towards the future, there is little reason to expect that older people will change their strong aging in place preferences. Consequently, it is important to understand the factors that contribute to their reluctance to move and both the advantages and disadvantages of their residential decisions. This analytical focus must obviously incorporate the assessments of professionals and experts, but it must also include the diverse and idiosyncratic voices of older people. The proposed residential normalcy theory offers a holistic framework to assess why older people feel differently about their places of residence, why they initiate different coping strategies, and why they are not equally successful alleviating or eliminating the incongruent aspects of their residential and care arrangements.
The authors have declared that no competing interests exist.
AldwinC, IgarashiH.2012. An ecological model of resilience in late life[M]//Hayslip B, Smith G C. Annual review of gerontology and geriatrics. New York: Springer Publishing Co., 115-130.
Everyday competence and everyday problem solving in aging adults: the role of physical and social context
[M]//Wahl H W, Scheidt R J, Windley P G. Annual review of gerontology and geriatrics, Vol. 23. Aging in context: socio-physical environments. New York:Springer, 130-166.
Golant SM.1984. A place to grow old: the meaning of environment in old age[M]. New York: Columbia University Press.
[17]
Golant SM.1998. Changing an older person's shelter and care setting: a model to explain personal and environmental outcomes[M]//Windley P G, Scheidt R J. Environment and aging theory: a focus on housing. New York: Greenwood Press:34-60.
Identifying living arrangements that heighten risk for loneliness in later life: evidence from the U.S. national social life, health, and aging project
[J]. Journal of Applied Gerontology, 30(4): 524-534.
Hall JS, Zautra AJ.2010. Indicators of community resilience: what are they, why bother[M]//Reich J W, Zautra A J, Hall J S. Handbook of adult resilience. New York: Guilford Press, 350-371.
KrauseN.2003. Neighborhoods, health, and well-being in later life[M]//Wahl H-W, Scheidt R J, Windley P G. Annual review of gerontology and geriatrics: focus on aging in context, socio-physical environments. New York: Springer Publishing:223-249.
Lieberman MA.1991. Relocation of the frail elderly[M]//Birrren J E, Lubben J E, Rowe J C, et al. The concept and measurement of quality of life in the frail elderly. New York: Academic Press:120-141.
MagaiC.2001. Emotions over the life span[M]//BirrenJ E, Schaie K W. Handbook of the psychology of aging. 5th ed. San Diego, CA: Academic Press:399-426.
Rubinstein RL.1998. The phenomenology of housing for older people[M]//Scheidt R J, Windley P G. Environment and aging theory: a focus on housing. Westport, CT: Greenwood Press, 89-110.
Torres-GilF, HoflandB.2012. Vulnerable populations[M]//Cisneros H, Dyer-Chamberlain M, Hickie J. Independent for life: homes and neighborhoods for an aging America. Austin, TX: University of Texas Press, 221-232.
The contributions of race, individual socioeconomic status, and neighborhood socioeconomic context on the self-rated health trajectories and mortality of older adults
United States: state housing profiles, 2011[R]. Washington, DC:
2
2011
... 第一,住房成本可能超出老年人的承受水平.据统计,住房支出占老年人家庭支出的35%,占最低收入家庭总支出的43%(Social Security Administration, 2013).住房成本主要包括房租、水电费、贷款利息、房产税和业主财产保险费.2011年, 65岁以上老年人中,61%的租房者和35%的购房者用于住房的花销占其家庭收入的30%以上,其中,约36%的租户和18%的房主每月支付的居住成本甚至超过其收入的50%(U.S. Department of Housing and Urban Development, 2013).部分老年人群体(包括低收入者、非裔和拉丁裔美国人、未婚女性和受教育程度低的人群)的住房负担非常沉重,仍在偿还抵押贷款的低收入老年业主尤其不堪重负(AARP Public Policy Institute, 2011).近年来,步入老年尚须偿还住房贷款的美国人比例较过去有所提高,根据2010年的一项统计,有54%的55~64岁、41%的65~74岁和24%的75岁以上的房主仍在偿还住房贷款(Trawinski, 2012). ...
... Some groups of older people have especially high dwelling expense burdens and include the poor, African Americans and Hispanics, unmarried women, and the less educated. Lower income older homeowners still paying off their mortgages are especially burdened(AARP Public Policy Institute, 2011). Older people in the United States today are much more likely to be still paying off their home loans than in the past. In 2010, this included 54% of age 55~64, 41% of age 65~74, and 24% of age 75 plus homeowners(Trawinski, 2012). ...
2
... (1) 他们是更具灵活性的个体(Skodol, 2010; Aldwin et al, 2012; Wiles et al, 2012b; Wild et al, 2013).他们具有的个性、价值观和人口统计学特征(年龄、职业、文化、收入等)激励和帮助其找到创造性和建设性的自我适应策略来应对逆境.例如,他们可能有更丰富的技巧去解决问题,或丰厚财力使其更容易承担额外成本.这些老年人过去的生活经历使其更有能力解决遇到的问题.他们可能具有信任他人和开放的个性,容易得到别人帮助和支持,因此会积极寻求解决问题的方案.他们也可能是更快乐的人,对生活具有乐观的看法,从而对自己的未来更有希望. ...
... The theory proposes three factors to explain why some older people have more enriched coping repertories(Fig.4). First, they will be more resilient individuals(Skodol, 2010; Aldwin et al, 2012; Wiles et al, 2012b; Wild et al, 2013). They will have personalities, values, and demographics that motivate and enable them to find creative and constructive adaptive strategies to deal with their adversity. For example, they may have stronger problem-solving skills or have financial resources that make it easier for them to tolerate the collateral costs connected with implementing their coping solutions. The past life experiences of these older individuals will have better prepared them to deal with their problems. They are likely to have personalities predisposing them to finding solutions because they are more trusting and open to receiving the help or supports of others. They are also likely to be happier persons who have optimistic outlooks on their lives and are therefore more hopeful about their futures. ...
The 'taking place' of health and wellbeing: towards non-representational theory
... Geographers have long recognized the importance of studying how people feel about the places where they live and conduct their activities(Rowles, 1978; Milligan, 2005; Andrews et al, 2013, 2014; Skinner et al, 2015). Similarly, psychologists have argued that the emotional reactions of individuals represent "the common core of human response to all types of environments”(Mehrabian, 1980). Life-span scholars have particularly recognized the motivational roles played by emotion as(Magai, 2001) emphasizes: ...
Re-spacing and re-placing gerontology: relationality and affect
... Geographers have long recognized the importance of studying how people feel about the places where they live and conduct their activities(Rowles, 1978; Milligan, 2005; Andrews et al, 2013, 2014; Skinner et al, 2015). Similarly, psychologists have argued that the emotional reactions of individuals represent "the common core of human response to all types of environments”(Mehrabian, 1980). Life-span scholars have particularly recognized the motivational roles played by emotion as(Magai, 2001) emphasizes: ...
Aging americans: stranded without options[R]. Washington, DC:
2
2004
... 第六,大量的美国老年人住在公共交通不能覆盖的人口稀疏的城市郊区或农村地区.当他们还能开车时,购物等日常活动尚无多大困难.然而随着年龄增大,开车变得不可能或不安全.许多上年纪的寡居老人也存在交通困难,因为她们再也不能依靠丈夫送自己到目的地(Mezuk et al, 2008; Connell et al, 2013).出行不便的老人不仅更少参加休闲或社交活动,而且会减少购物和看病的次数(Baily, 2004).一些老人搭便车或使用叫车服务,但如此一来他们就失去了自行或预先安排行程的自主性;在晚上或周末他们需要外出时更是困难重重. ...
... Sixth, large shares of older people in the United States occupy low-density cul-de-sac urban suburbs or population sparse rural areas where public transit is unavailable. When these residents could drive, they had little difficulty reaching their everyday goods and services. However, when they experience the physical or cognitive declines of aging, driving becomes impossible or unsafe. Many older widows also experience transportation difficulties because they can no longer rely on their husbands to drive them to their destinations(Mezuk et al, 2008; Connell et al, 2013). Lacking reliable transportation, older people not only engage in fewer recreational or social activities, but also curtail their visits to their grocery stores and doctors(Baily, 2004). ...
Do the rich flee from high state taxes? Evidence from federal estate tax returns[R]. Working Paper 10645. Cambridge, MA: National Bureau of
2
2004
... 经济因素对老年人就地养老行为的影响比较复杂.例如,并没有可靠证据证明老年人总是搬到生活成本或所得税、消费税、遗产税和房产税更低的地方(Duncombe et al, 2003; Bakija et al, 2004).如果经济因素是促使他们搬迁的主要动力,则应该有大量的老年人迁往他们成年子女的家里才对,因为在那儿他们可以免交房租.但事实并非如此.即使老年人的房屋开销负担偏重,他们的应对措施通常也不是搬到更便宜的住处,而是减少食物或保健等其他方面的花费、重新找一份工作或者提高信用卡的借贷额度(Pottow, 2011). ...
... Economic factors also contribute to the aging in place behaviors of older people but not in straightforward ways. There is no compelling evidence, for example, that older people always relocate to places with a lower cost of living or lower state income and sales taxes, inheritance and estate taxes(Duncombe et al, 2003; Bakija et al, 2004). If economic factors primarily motivated their moves, much larger numbers of older people would be relocating to the homes of their adult children where they could live rent-free. ...
The aging self: stabilizing and protective processes
2
1994
... 因此,居住常态理论认为,当老年人感觉自己处于居住舒适区或掌控区之外时,会使用人类发展理论家称之为适应(accommodative)或同化(assimilative)的应对策略(Brandtstädter et al, 1994).正如Golant(2015a)所说:“适应反应是指思维策略,老年人通过降低对环境的预期或愿望,从心理上淡化其住所缺点的影响,说服自己这些不完全合适的居住条件对他们的自尊心、自我认同或幸福感并没有那么重要.同化反应是指行动策略,即老年人改变他们对住宅环境的居住或使用方式,来改变其不适宜的设施或功能”. ...
... Consequently, the residential normalcy theory argues that when older people feel out of their residential comfort or residential mastery zones, they initiate what human development theorists identify as accommodative or assimilative forms of coping(Brandtstädter et al, 1994). As summarized elsewhere(Golant, 2015a): ...
Taking time seriously. A theory of socioemotional selectivity
2
1999
... 第四,对搬迁行动不感到过度紧张.不管现住所的问题有多严重,新居处安排有多理想,一些老年人还是会认为搬迁过程本身太累人、累心或费钱.例如,老年人可能不希望花费必要的精力去寻找新居住地或搬动物品.并且,老年人对自己存活期的预判可能会影响他们对这些代价是否值得的评价;如果他们觉得自己只能活不多的几年,就不情愿承担这些麻烦,因为他们认为这样做得不偿失(Carstensen et al, 1999). ...
... Fourth, however, serious their current housing problems or desirable their alternative residential arrangements, older people must not appraise the act of moving as overly stressful. Some older people will evaluate the moving process itself as too physically exhausting, psychologically demanding, or financially expensive. For example, older people may not want to spend the necessary energy searching for a new place of residence or to move their possessions. How close older people perceive their own death may influence how they evaluate these costs. If they feel they have only a few years left to live, they will be less willing to incur these costs because they will have only a relatively short time at a new destination to enjoy the compensating benefits(Carstensen et al, 1999). ...
Older adults' driving reduction and cessation: perspectives of adult children
2
2013
... 第六,大量的美国老年人住在公共交通不能覆盖的人口稀疏的城市郊区或农村地区.当他们还能开车时,购物等日常活动尚无多大困难.然而随着年龄增大,开车变得不可能或不安全.许多上年纪的寡居老人也存在交通困难,因为她们再也不能依靠丈夫送自己到目的地(Mezuk et al, 2008; Connell et al, 2013).出行不便的老人不仅更少参加休闲或社交活动,而且会减少购物和看病的次数(Baily, 2004).一些老人搭便车或使用叫车服务,但如此一来他们就失去了自行或预先安排行程的自主性;在晚上或周末他们需要外出时更是困难重重. ...
... Sixth, large shares of older people in the United States occupy low-density cul-de-sac urban suburbs or population sparse rural areas where public transit is unavailable. When these residents could drive, they had little difficulty reaching their everyday goods and services. However, when they experience the physical or cognitive declines of aging, driving becomes impossible or unsafe. Many older widows also experience transportation difficulties because they can no longer rely on their husbands to drive them to their destinations(Mezuk et al, 2008; Connell et al, 2013). Lacking reliable transportation, older people not only engage in fewer recreational or social activities, but also curtail their visits to their grocery stores and doctors(Baily, 2004). ...
2
... 第五,许多老年人害怕搬到一个无人认识和了解他们的新社区.他们不想反复告诉别人自己的个人背景和身份以获得认可和接受.他们同时也担心在与别人交流的过程中,谈起自己成功、丰富和有意义的过去时,自己会对生活的价值产生自我怀疑.而在他们居住已久的地方,朋友和邻居们很了解他们,能够欣赏或者至少容忍他们独特的行为或生活方式,他们也无需一直向别人介绍和证明自己(Cumming et al, 1962). ...
... Fifth, many older people dread the prospect of moving to a new community where nobody knows anything about their lives. They do not want to re-educate others about their personal backgrounds and identities as a way to gain recognition and acceptance. They worry too that in the process of communicating to others about their successful, productive, and meaningful pasts, they will begin to have their own self-doubts about the worthiness of their lives. Such conversations are unnecessary where they now live, because their friends and associates know them very well, appreciate or at least tolerate their distinctive behaviors or lifestyles, and they do not have to continually impress these significant others about their loyalties(Cumming et al, 1962). ...
... Importantly, when older people successfully cope with their difficulties, they do not necessarily "bounce back" to some original starting point or equilibrium(Davoudi, 2012). Consequently, when they again occupy places congruent with their needs and goals and have achieved residential normalcy, their new environments may have very different qualities and they may be conducting different activities or practicing different lifestyles. Consequently, older people may experience several new residential normals over their lives. As I emphasized earlier(Golant, 2015a): ...
Everyday competence and everyday problem solving in aging adults: the role of physical and social context
2
2003
... 第六,老年人对自己的隐私十分看重.他们希望自行决定跟谁交往、由谁来探望和看护自己.在自己的住宅或公寓内,他们可以很容易地掌控自己的交往活动;如果搬到其他地方,则难以维持这种自主权.因此,他们不愿搬到某个家庭成员家里或社会性的养老设施内.生活在一个可以控制自己社交活动的地方,对感到自己没有能力抵挡不诚实、不友好、讨厌或暴虐之人的老年人来说尤为重要(Diehl et al, 2003). ...
... Sixth, older people value highly their privacy. They want to decide with whom to communicate and who watches and monitors them. They fear that if they move elsewhere, they will have more difficulty maintaining this territorial control. They especially want to control their interpersonal interactions when in their dwellings or apartment buildings. These privacy concerns help explain their reluctance to relocate to the home of a family member or to a group residential facility, such as an assisted living development. Living in a place where they can control their social interactions are especially important for physically vulnerable older persons who feel less able to fend off dishonest, unfriendly, irritating, or abusive people(Diehl et al, 2003). ...
Place characteristics and residential location choice among the retirement-age population
2
2003
... 经济因素对老年人就地养老行为的影响比较复杂.例如,并没有可靠证据证明老年人总是搬到生活成本或所得税、消费税、遗产税和房产税更低的地方(Duncombe et al, 2003; Bakija et al, 2004).如果经济因素是促使他们搬迁的主要动力,则应该有大量的老年人迁往他们成年子女的家里才对,因为在那儿他们可以免交房租.但事实并非如此.即使老年人的房屋开销负担偏重,他们的应对措施通常也不是搬到更便宜的住处,而是减少食物或保健等其他方面的花费、重新找一份工作或者提高信用卡的借贷额度(Pottow, 2011). ...
... Economic factors also contribute to the aging in place behaviors of older people but not in straightforward ways. There is no compelling evidence, for example, that older people always relocate to places with a lower cost of living or lower state income and sales taxes, inheritance and estate taxes(Duncombe et al, 2003; Bakija et al, 2004). If economic factors primarily motivated their moves, much larger numbers of older people would be relocating to the homes of their adult children where they could live rent-free. ...
Household disbandment in later life
2
2004
... 第二,老年人对住所内的个人物品怀有强烈的感情.这些看起来仍然有用的东西不仅带给他们快乐,也是家庭财富的一部分,有的甚至可能还值点钱(Ekerdt et al, 2004).最重要的是,它们是往昔生活的物证,能够唤醒他们对过去的事件、场合及人际关系的记忆,帮助他们回忆生活中曾经的快乐场景和成就(Rubinstein, 1998).住在旧居里,他们就可以随时凭借这些与过往生活相关的物件去回想这些经历,去回味和享受自己曾经的成功. ...
... Second, older people have strong emotional attachments to the personal belongings in their dwellings. These possessions give them pleasure, still seem useful, are part of a family's legacy, and perhaps are even worth money(Ekerdt et al, 2004). Perhaps more importantly, they constitute archeological evidence or material signposts of their pasts that enable them to recall memories of events, occasions, and relationships. Thus, these possessions become catalysts for their reminiscing(or life reviews) helping them to recall the happy occasions in their lives and their successful achievements or accomplishments(Rubinstein, 1998). Moreover, they can choose when to recall these experiences and enjoy their pasts. They control this activity. ...
Older Americans 2012: key indicators of well-being
2
2012
... 身体健康状况变差,使老年人独立生活更加困难.当老年人接近80岁或年龄更高时,罹患各种慢性疾病(如高血压、关节炎、心脏病、癌症、糖尿病、哮喘、支气管炎)的风险会增加.他们将更难料理自身的健康问题,如服药、就医,洗澡、穿衣、吃饭、如厕、修饰、上下床、行走等日常生活活动(activities of daily living, ADLs),以及购物、烹调、做家务、服用药物、处理财务等工具性日常生活活动(instrumental activities of daily living, IADLs).即使是最基本的室内活动(如爬楼梯、使用壁柜等)也变得很不容易,在光滑的浴室地板上可能会摔倒;无法再开车,这使得他们前往社区商店和其他服务设施变得更加困难.患有老年认知障碍(其中最常见的是阿尔茨海默氏症)的老年人是最需要护理和帮助的群体.他们有情绪和行为障碍、容易四处游荡,需要不间断的监护和协助(Federal Interagency Forum on Aging-Related Statistics, 2012). ...
... Older persons who suffer from dementia, the most common being Alzheimer's disease, have some of the most demanding care and assistance needs. They require continual supervision and queuing to do everything, experience mood and behavioral disorders, and are prone to wandering(Federal Interagency Forum on Aging-Related Statistics, 2012). ...
... Subsequently, the great economic recession in the United States between 2007 and 2010 also produced some uniquely powerful aging in place influences. Over this period, housing values in most places declined sharply. Consequently, older people who might have seriously contemplated moving postponed these residential transitions because they were reluctant to realize equity returns far below their expectations. Additionally, because of the depressed economy and the unavailability of mortgage financing, there were few buyers for their homes. The stock market declines, smaller private pension benefits, and lower interest rate and dividend returns on their investment portfolios and savings accounts also increased the income insecurity of older people. Consequently, over this period, smaller shares of older people retired, but as a result they were restricted to residences near their job locations, a powerful moving constraint(Golant, 2008a). ...
... Older Americans hear a repetitive message from the print and internet media, experts in aging, long-term care providers, and family members who claim to know what is best for them. This "groupthink mindset" cajoles older people not to move but to cope with their health problems and impairments in their familiar dwellings. It considers any other solutions to be inferior, uninformed, or ill advised. The groupthink mindset argues that aging in place is the only right way to live out one's life(Golant, 2008a, 2009). ...
b. Low-income elderly homeowners in very old dwellings: the need for public policy debate
... A second set of problems result from older people occupying older housing. In 2011, more than a third of their dwellings were at least 50 years old(Golant, 2008b). As I summarized elsewhere: "Older buildings are especially at risk of having three categories of physical deficiencies: physical disrepair requiring equipment or infrastructure upgrades; outmoded physical design features; and physical features incompatible with the mobility or sensory declines of their occupants"(Golant, 2015b). These deficiencies influence the lives of older people in several ways: ...
... · They have slippery bathroom and shower area floors, and slick kitchen linoleum floors, that increase their risks of falling(Golant, 2008b). ...
Aging in place solutions for older Americans: groupthink responses not always in their best interests
... Older Americans hear a repetitive message from the print and internet media, experts in aging, long-term care providers, and family members who claim to know what is best for them. This "groupthink mindset" cajoles older people not to move but to cope with their health problems and impairments in their familiar dwellings. It considers any other solutions to be inferior, uninformed, or ill advised. The groupthink mindset argues that aging in place is the only right way to live out one's life(Golant, 2008a, 2009). ...
The quest for residential normalcy by older adults: relocation but one pathway
8
2011
... 对老年人可能经历的上述问题的分析表明,相关政策的制定者和实施者必须清楚,即有些老年人就地养老并不是因为他们觉得住在家里有多好,而是因为他们没有更好的选择,只好“被困在家里”(Torres-Gil et al, 2012).研究表明,在以下情况出现时老年人才会自愿决定搬迁(Golant, 2011). ...
... When older people experience these problems, practitioners and policymakers must be alert to the possibility that they are aging in place not because of the attractive features of their residences, but because they feel "stuck in place" and have no viable moving options(Torres-Gil et al, 2012). Older people typically decide to move—at least voluntarily—only if they have satisfied the following five conditions(Golant, 2011). ...
... To understand how older people judge their places of residence, this paper presents an overview of an earlier constructed residential normalcy theoretical model(Golant, 2011). It proposed that older people will occupy congruent residential settings that are consistent with their needs and goals when they report overall favorable or positive emotional experiences. ...
... The proposed theoretical model distinguishes two independent categories of emotional experiences: residential comfort and residential mastery emotional experiences. The model theorizes that older people achieve residential normalcy when they occupy places in which both sets of these experiences are overall favorable or positive(Golant, 2011). ...
... In the best case scenario, older people will be in their residential comfort zones when they get pleasure or enjoyment from their places of residence, do not feel hassled, and have good memories of their residential pasts; and they will be in their residential mastery zones when they feel competent and in control of their residential surroundings. When older persons are both in their residential comfort and residential mastery zones, they have achieved “residential normalcy.” These are places(Golant, 2011): ...
Age-friendly Communities: are we expecting too much[R] Institute for Montreal: Research on Public Policy.
... This messaging is also occurring at a time when older people in the United States have many private and public sector options to help them to age in place. They can physically modify their dwellings to make them more congruent with their aging bodies, obtain assistive devices(e.g., canes and walkers), install medical monitoring and home security technologies in their dwellings, and obtain personal assistance and care from an historically high number of home care providers(Golant, 2015b). So-called age-friendly buildings, neighborhoods, and communities offer older people a variety of volunteer-provided and price discounted services that make it easier for them to age in place(Golant, 2014). Numerous federal and state public policies target lower income older people and offer them property tax relief, home repair and modification solutions, and affordable home care assistance. However, as I emphasize below, these societal responses are often far from perfect solutions and are not available to all segments of America's old. ...
... The incomes of older people matter. The care and services offered by the private sector are usually only affordable to higher income older people; and public sector solutions—which often have waiting lists—are only available for those with sufficiently low incomes and few assets. Perhaps surprisingly, middle-income older people in the United States often have the most difficulty securing assistance because they cannot afford the high costs of private care, yet they are not poor enough to be eligible for most public sector sponsored programs(Golant, 2014a, Golant, 2015b). Certain older groups are more at risk of not receiving adequate long-term services and supports in their homes: unmarried women, those with lower incomes; and minority groups, such as African Americans and Hispanics. Older persons living in more service-deficient and isolated locations—in outlying suburban and rural communities—also have more limited service options(Newcomer et al, 2005). ...
a. Residential normalcy and the enriched coping repertoires ofsuccessfully aging older adults
... 按照居住常态模型理论,老年人需要开展第二次评估过程(Lazarus et al, 1984)以决定如何消除或缓解居住地的不适宜性(Golant, 2015a).这些评估使一些老年人比其他人采取了更成功的适应策略.该模型认为这些老年人具有更丰富的应对办法.也就是说,他们对什么是有效的应对策略有更清楚的认识,这使得他们能够及时、有效地处理问题(不管这些问题有多复杂),获得可行的解决方案.有效应对措施的标准是既不会使身、心和财力上产生负担,也不能与他们的生活方式相冲突,或强迫他们违背自己的价值观和信仰.采取这些应对策略产生的间接成本较低. ...
... Studies assessing whether older people occupy congruent residential settings are typically point-in-time or cross-sectional analyses. Consequently, most researchers of the housing conditions of older Americans prematurely end their analyses after they find that their sample of respondents occupy poor quality residential environments. The residential normalcy theory argues that this static perspective is unrealistic(Golant, 2015a). At various times over their lifetimes, older people may find themselves in residential situations that are inconsistent with their lifestyles or capabilities. However, this is not their end game. Human development theorists tell us that successfully aging older people do not give up attempting to find appropriate places to live and that their environmental incongruence may be a momentary occurrence. Rather, they proactively initiate coping behaviors—that is, they actively seek solutions to eliminate or alleviate their housing problems. ...
... Consequently, the residential normalcy theory argues that when older people feel out of their residential comfort or residential mastery zones, they initiate what human development theorists identify as accommodative or assimilative forms of coping(Brandtstädter et al, 1994). As summarized elsewhere(Golant, 2015a): ...
... Importantly, when older people successfully cope with their difficulties, they do not necessarily "bounce back" to some original starting point or equilibrium(Davoudi, 2012). Consequently, when they again occupy places congruent with their needs and goals and have achieved residential normalcy, their new environments may have very different qualities and they may be conducting different activities or practicing different lifestyles. Consequently, older people may experience several new residential normals over their lives. As I emphasized earlier(Golant, 2015a): ...
... The residential normalcy model theorizes that older people must engage in a secondary appraisal process(Lazarus et al, 1984) to decide on how they might eliminate or alleviate their incongruent places of residence(Golant, 2015a). However, these deliberations result in some older people initiating more successful adaptive strategies. The model argues that these persons have more enriched coping repertoires. That is, they will be more aware of coping strategies that they appraise as efficacious, enabling them to timely manage or successfully resolve their problems whatever their complexity; and these will be more viable or doable solutions. That is, older people will appraise these coping efforts as less physically burdensome, strenuous, financially overwhelming, or less likely to clash with their lifestyles or force them to violate their values or beliefs. To initiate these coping strategies, older people will incur lower collateral costs. ...
... 第五,邻里和社区发生的一些变化会令老年人感到不便.当一家喜欢的商店关闭、一位医生退休,或一条公共汽车线路停止服务,老年人就会感到自己的生活受到困扰.在一些没有活力的老城市、小城镇和农村,失去农业、制造业或能源领域工作的老年人经济上陷入困境.这些社区被称为“老人留守”的地方,因为年轻人口迁移别处寻求就业,留下的是失业的、受教育程度较低的人和老年人(Golant, 1984).这些地方可能出现社会秩序混乱(如犯罪、毒品、酗酒、破坏公物),建筑物废弃或破败.老年人一般会减少外出,因为独自外出缺乏安全感;并且,这些地方往往缺少休闲娱乐的条件(如公园、广场、图书馆和为老年人组织的活动),及保健和长期照护服务(Krause, 2003; Yao et al, 2008). ...
... This paper reviews the strong attractions of their current residences to explain the aging in place behaviors of older people, although the paucity of available and viable housing alternatives also explains their residential inertia. This overview also emphasizes that the residential arrangements of older people are often more than just places to live. When older people confront difficulties living independently, they often modify their dwellings to make it easier for them to cope with their chronic health problems and physical and cognitive limitations. Consequently, they might add grab-bars in their bathrooms, install raised toilet seats, add handrails to their staircases, or install an emergency response system to alert others when they fall. Their homes will also be frequented by both informal(e.g., family members) and formal(paid professionals or home care workers) caregivers who offer them a variety of health, rehabilitative, and supportive services. Because of these physical modifications and the provision of in-home assistance, the residences of older Americans have often become de facto care settings(Golant, 2015b). Consequently, when we study the quality of life of older Americans, we often must recognize that they are sometimes living in both residential and care environments. ...
... Six sets of social or psychological factors help explain older people's strong attractions to their current places of residence(Wiles et al, 2012a, Golant, 2015b). First, older people want to remain in familiar environments. Here they have more accurate, complete, and reliable cognitive maps of their surroundings. Consequently, they feel more confident and competent navigating around their dwellings, neighborhoods, and communities. If they lose electrical power, even in the dark they can safely find things in their dwellings. Similarly, they have good knowledge of where the stores, services, and transportation routes are in their communities and can satisfy their everyday needs with minimal mental and physical energy. In their familiar places, they have friends to share enjoyable social experiences and thus are less likely to feel alone. They are also more aware of who they can count on when they need assistance with their everyday needs—whether getting a ride to their doctors or assistance with their shopping. These older people reason that it would take years for them to establish such reliable connections in a new community. ...
... Confronted with these physical and mental declines, we might expect that older people would move to group residential care facilities(e.g., assisted living) or to the home of a family member to obtain more assistance. However, this is usually not the case. Rather, older people cope with their aging bodies by modifying their current dwellings, such as by adding grab bars, installing nonslip floors, or improving their dwelling's lighting. Alternatively, they make few adjustments to their accommodations and simply avoid the offensive aspects of their residences—for example, they live on the first floor of their two-story houses. When physical modifications are insufficient, they solicit the help from family members; or they take advantage of the home- and community-based services available in their community, some targeting low income older people(National Consumer Voice for Quality Long-Term Care, 2012, Golant, 2015b). ...
... This messaging is also occurring at a time when older people in the United States have many private and public sector options to help them to age in place. They can physically modify their dwellings to make them more congruent with their aging bodies, obtain assistive devices(e.g., canes and walkers), install medical monitoring and home security technologies in their dwellings, and obtain personal assistance and care from an historically high number of home care providers(Golant, 2015b). So-called age-friendly buildings, neighborhoods, and communities offer older people a variety of volunteer-provided and price discounted services that make it easier for them to age in place(Golant, 2014). Numerous federal and state public policies target lower income older people and offer them property tax relief, home repair and modification solutions, and affordable home care assistance. However, as I emphasize below, these societal responses are often far from perfect solutions and are not available to all segments of America's old. ...
... A second set of problems result from older people occupying older housing. In 2011, more than a third of their dwellings were at least 50 years old(Golant, 2008b). As I summarized elsewhere: "Older buildings are especially at risk of having three categories of physical deficiencies: physical disrepair requiring equipment or infrastructure upgrades; outmoded physical design features; and physical features incompatible with the mobility or sensory declines of their occupants"(Golant, 2015b). These deficiencies influence the lives of older people in several ways: ...
... The incomes of older people matter. The care and services offered by the private sector are usually only affordable to higher income older people; and public sector solutions—which often have waiting lists—are only available for those with sufficiently low incomes and few assets. Perhaps surprisingly, middle-income older people in the United States often have the most difficulty securing assistance because they cannot afford the high costs of private care, yet they are not poor enough to be eligible for most public sector sponsored programs(Golant, 2014a, Golant, 2015b). Certain older groups are more at risk of not receiving adequate long-term services and supports in their homes: unmarried women, those with lower incomes; and minority groups, such as African Americans and Hispanics. Older persons living in more service-deficient and isolated locations—in outlying suburban and rural communities—also have more limited service options(Newcomer et al, 2005). ...
... Paradoxically, there are also downsides if older people receive too much care in their homes. When family members serve as their caregivers, they often act more like professional workers than emotionally close significant others; and the introduction of assistive devices and medical equipment often makes the dwellings of older people look and operate more like an institution(e.g., a nursing home) than a residential setting(Golant, 2015b). ...
... Fifth, older people find themselves in neighborhoods and communities that have experienced undesirable physical or demographic changes. The lives of older people are disrupted when a favorite store closes, a doctor retires, or a bus service stops. Other communities—in older cities, small towns, and rural counties—decline economically because they have lost jobs in their agricultural, manufacturing, or energy sectors. Sometimes they are referred to as "aged left behind" localities, because younger populations migrate elsewhere seeking jobs and the unemployed, less educated, and older populations are left behind(Golant, 1984) . These places are more likely to have social disorders, such as crime, drug and alcohol use, and vandalism and have abandoned or physically rundown buildings. Older people in these locales tend to venture out less frequently, feel insecure walking alone, and they lack the supports of trusted neighbors. These places often lack recreational amenities(e.g., parks, public squares, libraries, and organized events for older people), but also healthcare and long-term care offerings(Krause, 2003; Yao et al, 2008). ...
... Academics and professionals often judge the quality of older people's housing by relying on their detached scientific or objective indicators. But older people do not always agree with these appraisals. Their considerations of the pros and cons of where they live depend on how they personally interpret and evaluate these indicators. A variety of individual attributes that have distinguished older people throughout their lives will influence these subjective assessments, including their personalities and demographics. Older people will also differently evaluate their current housing situations because of their past residential experiences. And their appraisals will depend also on whether they have incurred declines in their health and difficulties performing their ADLs and IADLs(Golant, 1998). ...
... Older people may not agree on what constitute the pleasurable or enjoyable aspects of their places of residence(Golant, 2015b): ...
Identifying living arrangements that heighten risk for loneliness in later life: evidence from the U.S. national social life, health, and aging project
2
2011
... 第四,高龄老年人很有可能独自生活.据统计,2010年美国65岁的老年人中,约19%的男性和37%的女性是独自居住;在七八十岁的老年人中独居比例更高(U.S. Department of Health and Human Services, 2012).因此,许多老年人受到孤独的折磨.例如,若配偶去世,老年人不仅失去了一个可以依赖的朋友、一个灵魂伴侣,更失去了帮助打理住所或提供交通便利的人.随着时间的推移,重要的朋友去世或者搬迁到其他地方,他们对一幢建筑、一个邻里或社区的眷恋会发生改变.当老年人外出活动能力下降导致无法参加社交活动时,孤独感便会油然而生.他们还会影响到其他老年人的社会行为,因为人们都不愿意经常跟那些比自己更衰弱的人在一起——和他们在一起乐趣不多,而且还时时提醒自己未来也会衰弱不堪.流行病学家发现,孤独的老年人身心不健康的风险更高,因为无人帮助他们应对健康和活动能力下降问题,或者缺乏可信任的人给予情感支持(Greenfield et al, 2011; Perissinotto et al, 2012). ...
... Epidemiologists report that older people who are lonely are at greater risk of experiencing other adverse physical and mental health outcomes because they lack persons to help them cope with their health problems or mobility declines or because they lack the emotional supports of trusted individuals(Greenfield et al, 2011; Perissinotto et al, 2012). ...
2
... (2) 具有丰富应对技能的老年人多居住在或可以搬到更具弹性的社区.这些社区很好地适应了帮助其老年居民应对挑战的过程,为居民提供了更多的机会和资源来实现其居住常态(Hall et al, 2010).在这些地方,老年人可以得到更多有趣或愉快的经历(如更多的朋友、有吸引力的休闲机会,或更少的住宅维修等的麻烦).这些地方提供了适合老年人生活方式和使用需求,价格实惠或设计精良的住宅或建筑物.此外,这些地方为身体衰弱的老年人提供更多的长期支持和服务,使他们能够应付自己的局限性和慢性健康问题,进而帮助其提升自我评价(感觉自己更有能力、更自主和更有控制力).这些社区有(来自公共、私有和非营利部门)思维更超前的领袖,能够认识到通过改善其财务资源、教育或培训、公民参与状况以及组织和解决问题的能力,从而帮助老年人的重要性. ...
... Second, older persons with enriched coping repertoires will occupy or can move to more resilient communities that have better adapted to the challenges faced by their older residents. These communities offer their residents more opportunities or resources for them to achieve their residential normalcy(Hall et al, 2010). In these locales, older people find more enjoyable or pleasurable place experiences(e.g., more friends, attractive recreational opportunities, or fewer dwelling maintenance hassles). These places offer more affordable or better designed dwellings or buildings that cater to the lifestyles and accessibility needs of older adults. Additionally, these places offer their physically vulnerable older occupants more long-term supports and services that enable them to cope with their limitations and chronic health problems and thus help them feel more competent, autonomous, and in control. These communities will have more forward thinking leaders(from the public, private, and nonprofit sectors) who recognize the importance of empowering older persons by improving their financial resources, education or training, civic engagement, and organizational and problem-solving skills. ...
Comparison of two modes of stress measurement: daily hassles and uplifts versus major life events
2
1981
... 居住舒适情感体验刻画了老年人对他们的住宅、邻里和社区环境感到愉快、舒适和满意程度.积极的情感体验包括:满足(vs 不满)、刺激(vs 无聊)、愉快(vs忧郁)、被认可(vs 被排斥)和高兴(vs 厌恶)等.同时,居住舒适情感体验也涉及到老年人是否受到生活中麻烦琐事的困扰,即“环境带给人的烦恼、沮丧、痛苦的情感体验”(Kanner et al, 1981).例如,铲雪,与讨厌的邻居或让人生气的工人打交道等.这类体验不仅仅来自于当前,对过去经历的活动和事件等的记忆,也会造成愉快(或不愉快)的情感体验. ...
... The first category, residential comfort experiences, captures the extent to which older people feel that their dwellings and their neighborhood and community environs are pleasurable, comfortable, and enjoyable places to live. When these experiences are positive, older people variously feel contented(vs. discontented), stimulated(vs. bored), cheerful(vs. glum), accepted(vs. rejected), and delighted(vs. disgusted). This category also captures whether older people are experiencing the hassles of life, "the irritating, frustrating, distressing demands that to some degree characterize everyday transactions with the environment"(Kanner et al, 1981). Examples include, shoveling snow, interacting with an annoying neighbor or an irritating staff person. Some experiences in this category are not a result of current environmental transactions, but rather are a product of past activities and events. These residential memories also constitute an important source of their pleasurable(or unpleasurable) experiences. ...
Long-term care: who gets it, who provides it, who pays, and how much
2
2010
... 第三,对存在健康问题和活动受到限制的老年人来说,就地养老使他们往往得不到适当的帮助和照顾.家人不一定随时都能提供帮助,收费护工也可能负担不起(Kaye et al, 2010).而且家人可能并无护理经验或专门训练,偶尔甚至可能出现虐老行为.而私营部门专业人士(如老年科医生、护士、康复专家)供不应求;负责家政和照顾老人的工作人员又常常未经足够培训,或者在夜晚和周末不提供服务(Stone et al, 2010). ...
... Third, when older people with health problems and mobility limitations opt to age in place in their current dwellings, they often do not get sufficient or good quality assistance and care. Some older people cannot always count on help from their family members or alternatively afford the care offered by paid workers(Kaye et al, 2010). Even when family members are available, they may have little care experience or training, and sometimes may even be guilty of abusive behavior. Private sector professionals(e.g., geriatric doctors, nurses, rehab specialists) are often in short supply; and hands-on(direct care) workers assisting with homemaking and self-care tasks often have insufficient training or are unavailable when needed—e.g., nights and weekends(Stone et al, 2010). ...
... Third, older people are often proud of their current dwellings, neighborhoods, or communities. Consequently, their built or material settings offer evidence to their friends and families that they are accomplished individuals who have lived successful lives. The opinions of others may be especially important to older widows who owe their current socioeconomic status and material possessions to the accomplishments of their now deceased husbands. These older women fear that if they vacate their current houses, they would abandon their only material evidence that they had competent and worthy lives(Kemper, 1978). ...
... Fourth, many older persons stay put because they are averse to experiencing novel events and activities. They enjoy the sameness or continuity of their activities, events, and environments. They fear that in a new place of residence they would continually have surprising, unsettling, and unpredictable experiences(Klapp, 1986). Rather, they favor remaining in places where they can enjoy their ritualistic activities of everyday living—whether watching their TV programs in their favorite rooms, walking their dogs, participating in Sunday church services, or meeting at a familiar restaurant with good friends. ...
2
... 第五,邻里和社区发生的一些变化会令老年人感到不便.当一家喜欢的商店关闭、一位医生退休,或一条公共汽车线路停止服务,老年人就会感到自己的生活受到困扰.在一些没有活力的老城市、小城镇和农村,失去农业、制造业或能源领域工作的老年人经济上陷入困境.这些社区被称为“老人留守”的地方,因为年轻人口迁移别处寻求就业,留下的是失业的、受教育程度较低的人和老年人(Golant, 1984).这些地方可能出现社会秩序混乱(如犯罪、毒品、酗酒、破坏公物),建筑物废弃或破败.老年人一般会减少外出,因为独自外出缺乏安全感;并且,这些地方往往缺少休闲娱乐的条件(如公园、广场、图书馆和为老年人组织的活动),及保健和长期照护服务(Krause, 2003; Yao et al, 2008). ...
... Fifth, older people find themselves in neighborhoods and communities that have experienced undesirable physical or demographic changes. The lives of older people are disrupted when a favorite store closes, a doctor retires, or a bus service stops. Other communities—in older cities, small towns, and rural counties—decline economically because they have lost jobs in their agricultural, manufacturing, or energy sectors. Sometimes they are referred to as "aged left behind" localities, because younger populations migrate elsewhere seeking jobs and the unemployed, less educated, and older populations are left behind(Golant, 1984) . These places are more likely to have social disorders, such as crime, drug and alcohol use, and vandalism and have abandoned or physically rundown buildings. Older people in these locales tend to venture out less frequently, feel insecure walking alone, and they lack the supports of trusted neighbors. These places often lack recreational amenities(e.g., parks, public squares, libraries, and organized events for older people), but also healthcare and long-term care offerings(Krause, 2003; Yao et al, 2008). ...
The psychology of control
2
1983
... (3) 有丰富应对技能的老年人通常自主决定居住和护理事务或自愿将这些决策责任转交给他们信任的人.对经历身体衰退和认知下降的老年人来说,能自主选择自己的应对方案显得更加具有挑战性.在此情况下,成年子女或聘请的专业人士经常试图强迫老年人接受他们的居住和保健选择.然而,有证据表明,当老年人对自己的决策失去控制,或对自己居住和医疗事务的决策人的动机不信任时,其对生活质量的体验将更为负面(Langer et al, 1983; Lieberman, 1991; Morgan et al, 2013). ...
... And third, older people with more enriched coping repertoires typically make their own residential and care decisions, or have voluntarily shifted these decision-making responsibilities to persons they trust. Being able to select their own coping options becomes more challenging for older people who have experienced physical and cognitive declines. In these instances, their adult children or hired professionals often try to compel them to accept their residential and care choices. However, evidence shows that when older people lose control over their decision-making or do not trust the motives of those making their housing and care decisions, they experience more negative quality of life outcomes(Langer et al, 1983; Lieberman, 1991; Morgan et al, 2013). ...
2
... 按照居住常态模型理论,老年人需要开展第二次评估过程(Lazarus et al, 1984)以决定如何消除或缓解居住地的不适宜性(Golant, 2015a).这些评估使一些老年人比其他人采取了更成功的适应策略.该模型认为这些老年人具有更丰富的应对办法.也就是说,他们对什么是有效的应对策略有更清楚的认识,这使得他们能够及时、有效地处理问题(不管这些问题有多复杂),获得可行的解决方案.有效应对措施的标准是既不会使身、心和财力上产生负担,也不能与他们的生活方式相冲突,或强迫他们违背自己的价值观和信仰.采取这些应对策略产生的间接成本较低. ...
... The residential normalcy model theorizes that older people must engage in a secondary appraisal process(Lazarus et al, 1984) to decide on how they might eliminate or alleviate their incongruent places of residence(Golant, 2015a). However, these deliberations result in some older people initiating more successful adaptive strategies. The model argues that these persons have more enriched coping repertoires. That is, they will be more aware of coping strategies that they appraise as efficacious, enabling them to timely manage or successfully resolve their problems whatever their complexity; and these will be more viable or doable solutions. That is, older people will appraise these coping efforts as less physically burdensome, strenuous, financially overwhelming, or less likely to clash with their lifestyles or force them to violate their values or beliefs. To initiate these coping strategies, older people will incur lower collateral costs. ...
2
... (3) 有丰富应对技能的老年人通常自主决定居住和护理事务或自愿将这些决策责任转交给他们信任的人.对经历身体衰退和认知下降的老年人来说,能自主选择自己的应对方案显得更加具有挑战性.在此情况下,成年子女或聘请的专业人士经常试图强迫老年人接受他们的居住和保健选择.然而,有证据表明,当老年人对自己的决策失去控制,或对自己居住和医疗事务的决策人的动机不信任时,其对生活质量的体验将更为负面(Langer et al, 1983; Lieberman, 1991; Morgan et al, 2013). ...
... And third, older people with more enriched coping repertoires typically make their own residential and care decisions, or have voluntarily shifted these decision-making responsibilities to persons they trust. Being able to select their own coping options becomes more challenging for older people who have experienced physical and cognitive declines. In these instances, their adult children or hired professionals often try to compel them to accept their residential and care choices. However, evidence shows that when older people lose control over their decision-making or do not trust the motives of those making their housing and care decisions, they experience more negative quality of life outcomes(Langer et al, 1983; Lieberman, 1991; Morgan et al, 2013). ...
... Geographers have long recognized the importance of studying how people feel about the places where they live and conduct their activities(Rowles, 1978; Milligan, 2005; Andrews et al, 2013, 2014; Skinner et al, 2015). Similarly, psychologists have argued that the emotional reactions of individuals represent "the common core of human response to all types of environments”(Mehrabian, 1980). Life-span scholars have particularly recognized the motivational roles played by emotion as(Magai, 2001) emphasizes: ...
Emerging cohort trends in housing debt and home equity
2
2006
... 与经济学理论背道而驰的事实是,老年人通常不会把自己的房屋兑换成现金来支付自己的开支,即不愿意消费他们的房产资源.例如,2011年美国仅有7%的65岁以上的老年房主申请房屋净值贷款(equity loans),只有大约2%的老年房主有反向抵押贷款(reverse mortgages,是一种以老年人的房产作为抵押的联邦担保贷款).相反,他们通常把房产当作支付未来潜在的大笔医疗和长期照护费的资金来源,或想要把房产作为财富转移给子女.老年业主一般不愿意出售自己的房屋,因为担心如果改为租房居住,将面临租金上涨的风险(Masnick et al, 2006). ...
... Contrary to economic theory, older people are usually reluctant to use(cash out) their dwellings' equity(home value less mortgage loan debt) to help pay for their housing expenses—that is, consume their housing wealth. In 2011, for example, only 7% of homeowners age 65 and older had home equity loans, and only about 2% had reverse mortgages(federally insured loans that enable older people to receive a substantial amount of their home's equity in the form of cash advances). Rather, older people usually treat the equity in their dwellings as a "rainy day" funding source to cover their potentially large future medical and long-term care expenses or as a way to transfer their wealth to their children. Older homeowners also fear that if they become renters, they will risk having continual and unexpected rent increases(Masnick et al, 2006). ...
Basic dimensions for a general psychological theory: implications for personality, social, environmental, and developmental studies
... Geographers have long recognized the importance of studying how people feel about the places where they live and conduct their activities(Rowles, 1978; Milligan, 2005; Andrews et al, 2013, 2014; Skinner et al, 2015). Similarly, psychologists have argued that the emotional reactions of individuals represent "the common core of human response to all types of environments”(Mehrabian, 1980). Life-span scholars have particularly recognized the motivational roles played by emotion as(Magai, 2001) emphasizes: ...
Social integration and social support among older adults following driving cessation
2
2008
... 第六,大量的美国老年人住在公共交通不能覆盖的人口稀疏的城市郊区或农村地区.当他们还能开车时,购物等日常活动尚无多大困难.然而随着年龄增大,开车变得不可能或不安全.许多上年纪的寡居老人也存在交通困难,因为她们再也不能依靠丈夫送自己到目的地(Mezuk et al, 2008; Connell et al, 2013).出行不便的老人不仅更少参加休闲或社交活动,而且会减少购物和看病的次数(Baily, 2004).一些老人搭便车或使用叫车服务,但如此一来他们就失去了自行或预先安排行程的自主性;在晚上或周末他们需要外出时更是困难重重. ...
... Sixth, large shares of older people in the United States occupy low-density cul-de-sac urban suburbs or population sparse rural areas where public transit is unavailable. When these residents could drive, they had little difficulty reaching their everyday goods and services. However, when they experience the physical or cognitive declines of aging, driving becomes impossible or unsafe. Many older widows also experience transportation difficulties because they can no longer rely on their husbands to drive them to their destinations(Mezuk et al, 2008; Connell et al, 2013). Lacking reliable transportation, older people not only engage in fewer recreational or social activities, but also curtail their visits to their grocery stores and doctors(Baily, 2004). ...
From home to 'home': situating emotions within the caregiving experience
... Geographers have long recognized the importance of studying how people feel about the places where they live and conduct their activities(Rowles, 1978; Milligan, 2005; Andrews et al, 2013, 2014; Skinner et al, 2015). Similarly, psychologists have argued that the emotional reactions of individuals represent "the common core of human response to all types of environments”(Mehrabian, 1980). Life-span scholars have particularly recognized the motivational roles played by emotion as(Magai, 2001) emphasizes: ...
Transferring control to others: process and meaning for older adults in assisted living
2
2013
... (3) 有丰富应对技能的老年人通常自主决定居住和护理事务或自愿将这些决策责任转交给他们信任的人.对经历身体衰退和认知下降的老年人来说,能自主选择自己的应对方案显得更加具有挑战性.在此情况下,成年子女或聘请的专业人士经常试图强迫老年人接受他们的居住和保健选择.然而,有证据表明,当老年人对自己的决策失去控制,或对自己居住和医疗事务的决策人的动机不信任时,其对生活质量的体验将更为负面(Langer et al, 1983; Lieberman, 1991; Morgan et al, 2013). ...
... And third, older people with more enriched coping repertoires typically make their own residential and care decisions, or have voluntarily shifted these decision-making responsibilities to persons they trust. Being able to select their own coping options becomes more challenging for older people who have experienced physical and cognitive declines. In these instances, their adult children or hired professionals often try to compel them to accept their residential and care choices. However, evidence shows that when older people lose control over their decision-making or do not trust the motives of those making their housing and care decisions, they experience more negative quality of life outcomes(Langer et al, 1983; Lieberman, 1991; Morgan et al, 2013). ...
Consumer perspectives on quality home care
2
2012
... 与我们想象中不同,身体和精神上日益衰退的老年人往往不会迁往专门养老设施或某个家庭成员家里以获得更多的帮助.他们通常通过对住宅设施做一些改变以满足身体需要,如增加扶手、安装防滑地板、改善照明条件,或搬到一层的房间居住.当这些调整仍然不够时,他们会寻求家人的帮助,或者利用社区提供的服务,其中部分服务是专门针对低收入老年人的(National Consumer Voice for Quality Long-Term Care, 2012; Golant, 2015b). ...
... Confronted with these physical and mental declines, we might expect that older people would move to group residential care facilities(e.g., assisted living) or to the home of a family member to obtain more assistance. However, this is usually not the case. Rather, older people cope with their aging bodies by modifying their current dwellings, such as by adding grab bars, installing nonslip floors, or improving their dwelling's lighting. Alternatively, they make few adjustments to their accommodations and simply avoid the offensive aspects of their residences—for example, they live on the first floor of their two-story houses. When physical modifications are insufficient, they solicit the help from family members; or they take advantage of the home- and community-based services available in their community, some targeting low income older people(National Consumer Voice for Quality Long-Term Care, 2012, Golant, 2015b). ...
Living quarters and unmet need for personal care assistance among adults with disabilities
2
2005
... 老年人收入水平是决定就地养老质量的重要因素.私营部门提供的照护和服务通常只有经济收入较高的老年人才负担得起,而公共部门提供的价格优惠的服务需要排队等待,并且只有那些收入足够低、没有任何资产的老人才能得到.所以,美国中等收入的老年人最无保障,因为他们既负担不起昂贵的私人保健费用,又没穷到有资格享受大多数公共部门资助项目的程度(Golant, 2015b).某些特定群体如未婚女性、低收入者以及少数族裔(如非裔和拉丁裔)更是难以得到足够的居家服务和支持,同时生活在偏远郊区和乡村社区的老年人可获得的服务也非常有限(Newcomer et al, 2005).另一方面,老年人在家中受到太多照顾也未必什么都好.当家庭成员充当照护者时,就会变得更像是职业护工,而不再是情感亲密、地位特殊的家人;辅助设施和医疗设备往往使老年人的住所更像一个养老机构而不是家(Golant, 2015b). ...
... The incomes of older people matter. The care and services offered by the private sector are usually only affordable to higher income older people; and public sector solutions—which often have waiting lists—are only available for those with sufficiently low incomes and few assets. Perhaps surprisingly, middle-income older people in the United States often have the most difficulty securing assistance because they cannot afford the high costs of private care, yet they are not poor enough to be eligible for most public sector sponsored programs(Golant, 2014a, Golant, 2015b). Certain older groups are more at risk of not receiving adequate long-term services and supports in their homes: unmarried women, those with lower incomes; and minority groups, such as African Americans and Hispanics. Older persons living in more service-deficient and isolated locations—in outlying suburban and rural communities—also have more limited service options(Newcomer et al, 2005). ...
Loneliness in older persons: a predictor of functional decline and death
2
2012
... 第四,高龄老年人很有可能独自生活.据统计,2010年美国65岁的老年人中,约19%的男性和37%的女性是独自居住;在七八十岁的老年人中独居比例更高(U.S. Department of Health and Human Services, 2012).因此,许多老年人受到孤独的折磨.例如,若配偶去世,老年人不仅失去了一个可以依赖的朋友、一个灵魂伴侣,更失去了帮助打理住所或提供交通便利的人.随着时间的推移,重要的朋友去世或者搬迁到其他地方,他们对一幢建筑、一个邻里或社区的眷恋会发生改变.当老年人外出活动能力下降导致无法参加社交活动时,孤独感便会油然而生.他们还会影响到其他老年人的社会行为,因为人们都不愿意经常跟那些比自己更衰弱的人在一起——和他们在一起乐趣不多,而且还时时提醒自己未来也会衰弱不堪.流行病学家发现,孤独的老年人身心不健康的风险更高,因为无人帮助他们应对健康和活动能力下降问题,或者缺乏可信任的人给予情感支持(Greenfield et al, 2011; Perissinotto et al, 2012). ...
... Epidemiologists report that older people who are lonely are at greater risk of experiencing other adverse physical and mental health outcomes because they lack persons to help them cope with their health problems or mobility declines or because they lack the emotional supports of trusted individuals(Greenfield et al, 2011; Perissinotto et al, 2012). ...
The rise in elder bankruptcy filings and failure of U.S. bankruptcy law
2
2011
... 经济因素对老年人就地养老行为的影响比较复杂.例如,并没有可靠证据证明老年人总是搬到生活成本或所得税、消费税、遗产税和房产税更低的地方(Duncombe et al, 2003; Bakija et al, 2004).如果经济因素是促使他们搬迁的主要动力,则应该有大量的老年人迁往他们成年子女的家里才对,因为在那儿他们可以免交房租.但事实并非如此.即使老年人的房屋开销负担偏重,他们的应对措施通常也不是搬到更便宜的住处,而是减少食物或保健等其他方面的花费、重新找一份工作或者提高信用卡的借贷额度(Pottow, 2011). ...
... Even when older people occupy dwellings with burdensome housing expenses, they often cope not by moving to less expensive accommodations, but by cutting back on what they spend on other items(e.g., food or health care), by returning to work, or alternatively by increasing their credit card debt(Pottow, 2011). ...
... Geographers have long recognized the importance of studying how people feel about the places where they live and conduct their activities(Rowles, 1978; Milligan, 2005; Andrews et al, 2013, 2014; Skinner et al, 2015). Similarly, psychologists have argued that the emotional reactions of individuals represent "the common core of human response to all types of environments”(Mehrabian, 1980). Life-span scholars have particularly recognized the motivational roles played by emotion as(Magai, 2001) emphasizes: ...
2
... 第二,老年人对住所内的个人物品怀有强烈的感情.这些看起来仍然有用的东西不仅带给他们快乐,也是家庭财富的一部分,有的甚至可能还值点钱(Ekerdt et al, 2004).最重要的是,它们是往昔生活的物证,能够唤醒他们对过去的事件、场合及人际关系的记忆,帮助他们回忆生活中曾经的快乐场景和成就(Rubinstein, 1998).住在旧居里,他们就可以随时凭借这些与过往生活相关的物件去回想这些经历,去回味和享受自己曾经的成功. ...
... Second, older people have strong emotional attachments to the personal belongings in their dwellings. These possessions give them pleasure, still seem useful, are part of a family's legacy, and perhaps are even worth money(Ekerdt et al, 2004). Perhaps more importantly, they constitute archeological evidence or material signposts of their pasts that enable them to recall memories of events, occasions, and relationships. Thus, these possessions become catalysts for their reminiscing(or life reviews) helping them to recall the happy occasions in their lives and their successful achievements or accomplishments(Rubinstein, 1998). Moreover, they can choose when to recall these experiences and enjoy their pasts. They control this activity. ...
Geographies of ageing: progress and possibilities after two decades of change
... Geographers have long recognized the importance of studying how people feel about the places where they live and conduct their activities(Rowles, 1978; Milligan, 2005; Andrews et al, 2013, 2014; Skinner et al, 2015). Similarly, psychologists have argued that the emotional reactions of individuals represent "the common core of human response to all types of environments”(Mehrabian, 1980). Life-span scholars have particularly recognized the motivational roles played by emotion as(Magai, 2001) emphasizes: ...
... The theory proposes three factors to explain why some older people have more enriched coping repertories(Fig.4). First, they will be more resilient individuals(Skodol, 2010; Aldwin et al, 2012; Wiles et al, 2012b; Wild et al, 2013). They will have personalities, values, and demographics that motivate and enable them to find creative and constructive adaptive strategies to deal with their adversity. For example, they may have stronger problem-solving skills or have financial resources that make it easier for them to tolerate the collateral costs connected with implementing their coping solutions. The past life experiences of these older individuals will have better prepared them to deal with their problems. They are likely to have personalities predisposing them to finding solutions because they are more trusting and open to receiving the help or supports of others. They are also likely to be happier persons who have optimistic outlooks on their lives and are therefore more hopeful about their futures. ...
1
... (1) 他们是更具灵活性的个体(Skodol, 2010; Aldwin et al, 2012; Wiles et al, 2012b; Wild et al, 2013).他们具有的个性、价值观和人口统计学特征(年龄、职业、文化、收入等)激励和帮助其找到创造性和建设性的自我适应策略来应对逆境.例如,他们可能有更丰富的技巧去解决问题,或丰厚财力使其更容易承担额外成本.这些老年人过去的生活经历使其更有能力解决遇到的问题.他们可能具有信任他人和开放的个性,容易得到别人帮助和支持,因此会积极寻求解决问题的方案.他们也可能是更快乐的人,对生活具有乐观的看法,从而对自己的未来更有希望. ...
Expenditures of the aged chartbook, 2010
2
2013
... 第一,住房成本可能超出老年人的承受水平.据统计,住房支出占老年人家庭支出的35%,占最低收入家庭总支出的43%(Social Security Administration, 2013).住房成本主要包括房租、水电费、贷款利息、房产税和业主财产保险费.2011年, 65岁以上老年人中,61%的租房者和35%的购房者用于住房的花销占其家庭收入的30%以上,其中,约36%的租户和18%的房主每月支付的居住成本甚至超过其收入的50%(U.S. Department of Housing and Urban Development, 2013).部分老年人群体(包括低收入者、非裔和拉丁裔美国人、未婚女性和受教育程度低的人群)的住房负担非常沉重,仍在偿还抵押贷款的低收入老年业主尤其不堪重负(AARP Public Policy Institute, 2011).近年来,步入老年尚须偿还住房贷款的美国人比例较过去有所提高,根据2010年的一项统计,有54%的55~64岁、41%的65~74岁和24%的75岁以上的房主仍在偿还住房贷款(Trawinski, 2012). ...
... First, older people are sometimes overburdened by their housing costs, which constitute 35% of their household expenditures, and 43% of the expenditures of those in the lowest income quartile(Social Security Administration, 2013).These costs primarily include the rent and utilities of renters and the mortgage payments, property taxes, and property insurance of owners. In 2011, 61% of renters and 35% of homeowners age 65 and older paid more than 30% of their household incomes on these housing expenses. About 36% of renters and 18% of owners paid monthly dwelling costs that were more than 50% of their incomes(U.S. Department of Housing and Urban Development, 2013). ...
Improving the long-term care workforce serving older adults
2
2010
... 第三,对存在健康问题和活动受到限制的老年人来说,就地养老使他们往往得不到适当的帮助和照顾.家人不一定随时都能提供帮助,收费护工也可能负担不起(Kaye et al, 2010).而且家人可能并无护理经验或专门训练,偶尔甚至可能出现虐老行为.而私营部门专业人士(如老年科医生、护士、康复专家)供不应求;负责家政和照顾老人的工作人员又常常未经足够培训,或者在夜晚和周末不提供服务(Stone et al, 2010). ...
... Third, when older people with health problems and mobility limitations opt to age in place in their current dwellings, they often do not get sufficient or good quality assistance and care. Some older people cannot always count on help from their family members or alternatively afford the care offered by paid workers(Kaye et al, 2010). Even when family members are available, they may have little care experience or training, and sometimes may even be guilty of abusive behavior. Private sector professionals(e.g., geriatric doctors, nurses, rehab specialists) are often in short supply; and hands-on(direct care) workers assisting with homemaking and self-care tasks often have insufficient training or are unavailable when needed—e.g., nights and weekends(Stone et al, 2010). ...
2
... 对老年人可能经历的上述问题的分析表明,相关政策的制定者和实施者必须清楚,即有些老年人就地养老并不是因为他们觉得住在家里有多好,而是因为他们没有更好的选择,只好“被困在家里”(Torres-Gil et al, 2012).研究表明,在以下情况出现时老年人才会自愿决定搬迁(Golant, 2011). ...
... When older people experience these problems, practitioners and policymakers must be alert to the possibility that they are aging in place not because of the attractive features of their residences, but because they feel "stuck in place" and have no viable moving options(Torres-Gil et al, 2012). Older people typically decide to move—at least voluntarily—only if they have satisfied the following five conditions(Golant, 2011). ...
Nightmare on main street: older Americans and the mortgage market crisis[R]. Washington, DC:
2
2012
... 第一,住房成本可能超出老年人的承受水平.据统计,住房支出占老年人家庭支出的35%,占最低收入家庭总支出的43%(Social Security Administration, 2013).住房成本主要包括房租、水电费、贷款利息、房产税和业主财产保险费.2011年, 65岁以上老年人中,61%的租房者和35%的购房者用于住房的花销占其家庭收入的30%以上,其中,约36%的租户和18%的房主每月支付的居住成本甚至超过其收入的50%(U.S. Department of Housing and Urban Development, 2013).部分老年人群体(包括低收入者、非裔和拉丁裔美国人、未婚女性和受教育程度低的人群)的住房负担非常沉重,仍在偿还抵押贷款的低收入老年业主尤其不堪重负(AARP Public Policy Institute, 2011).近年来,步入老年尚须偿还住房贷款的美国人比例较过去有所提高,根据2010年的一项统计,有54%的55~64岁、41%的65~74岁和24%的75岁以上的房主仍在偿还住房贷款(Trawinski, 2012). ...
... Some groups of older people have especially high dwelling expense burdens and include the poor, African Americans and Hispanics, unmarried women, and the less educated. Lower income older homeowners still paying off their mortgages are especially burdened(AARP Public Policy Institute, 2011). Older people in the United States today are much more likely to be still paying off their home loans than in the past. In 2010, this included 54% of age 55~64, 41% of age 65~74, and 24% of age 75 plus homeowners(Trawinski, 2012). ...
A profile of older Americans: 2012[R]. Washington, DC: U.S. Department of Health and Human Services, Administration on
2
2012
... 第四,高龄老年人很有可能独自生活.据统计,2010年美国65岁的老年人中,约19%的男性和37%的女性是独自居住;在七八十岁的老年人中独居比例更高(U.S. Department of Health and Human Services, 2012).因此,许多老年人受到孤独的折磨.例如,若配偶去世,老年人不仅失去了一个可以依赖的朋友、一个灵魂伴侣,更失去了帮助打理住所或提供交通便利的人.随着时间的推移,重要的朋友去世或者搬迁到其他地方,他们对一幢建筑、一个邻里或社区的眷恋会发生改变.当老年人外出活动能力下降导致无法参加社交活动时,孤独感便会油然而生.他们还会影响到其他老年人的社会行为,因为人们都不愿意经常跟那些比自己更衰弱的人在一起——和他们在一起乐趣不多,而且还时时提醒自己未来也会衰弱不堪.流行病学家发现,孤独的老年人身心不健康的风险更高,因为无人帮助他们应对健康和活动能力下降问题,或者缺乏可信任的人给予情感支持(Greenfield et al, 2011; Perissinotto et al, 2012). ...
... Fourth, at higher chronological ages, people are more likely to live alone. In 2010, about 19% of men and 37% of women age 65 and older lived alone and these percentages are higher for those in their 70s and 80s(U.S. Department of Health and Human Services, 2012). Consequently, many older people feel lonely and isolated. With the death of a spouse, for example, the older person can no longer count on a trusted confidant, a soul mate, or more practically, someone who had helped them maintain their dwelling or provided transportation. Over time, the social desirability of a building, neighborhood, or community changes after valued friends die or move away to other locations. Loneliness is also a consequence of older people experiencing mobility declines that prevent them from participating in social activities. Sadly, these declines also influence the social behaviors of other older persons. They often are reluctant to engage in activities with those who they perceive as more vulnerable than themselves, because they are no longer fun to be with or because they remind them of their own vulnerable futures. ...
American housing survey for the United States: 2011[R]. Washington, DC: U.S
4
2013
... 绝大多数(93%)超过65岁的美国老年人居住在普通的住宅和社区,而不是专门规划和建设的养老机构如养老院里.他们大都希望尽可能延长在当前住所居留的时间——即就地养老,拥有自己住房的老年人(占比高达79%)更是如此.约55%的美国老年人在同一个地方居住长达20年以上.有些人即使搬迁,一般也不会搬得太远,通常仍是在同一个州的同一个县境内(U.S. Department of Housing and Urban Development, 2013).甚至当他们在财务、健康、婚姻状况等方面经历重大变故而不得不开始新的生活方式,或者其居住环境大大改变以后,许多老年人还是希望持续这种就地养老的生活方式. ...
... 第一,住房成本可能超出老年人的承受水平.据统计,住房支出占老年人家庭支出的35%,占最低收入家庭总支出的43%(Social Security Administration, 2013).住房成本主要包括房租、水电费、贷款利息、房产税和业主财产保险费.2011年, 65岁以上老年人中,61%的租房者和35%的购房者用于住房的花销占其家庭收入的30%以上,其中,约36%的租户和18%的房主每月支付的居住成本甚至超过其收入的50%(U.S. Department of Housing and Urban Development, 2013).部分老年人群体(包括低收入者、非裔和拉丁裔美国人、未婚女性和受教育程度低的人群)的住房负担非常沉重,仍在偿还抵押贷款的低收入老年业主尤其不堪重负(AARP Public Policy Institute, 2011).近年来,步入老年尚须偿还住房贷款的美国人比例较过去有所提高,根据2010年的一项统计,有54%的55~64岁、41%的65~74岁和24%的75岁以上的房主仍在偿还住房贷款(Trawinski, 2012). ...
... The majority of older Americans in their mid-60s and older(93%) occupy ordinary dwellings and community settings as opposed to purposively planned and developed residential care facilities, such as assisted living developments or nursing homes. They also strongly prefer to remain as longtime residents in their current dwellings, that is, to age in place, especially the 79% who are homeowners. About 55% of the U.S. older population has lived at the same address for 20 or more years. Moreover, even when they do move, their new addresses are usually a short distance away, often within the same counties of their states(U.S. Department of Housing and Urban Development, 2013). These residential inertia patterns often persist even after older people experience significant changes in their financial, health, and marital status, embark on new lifestyles, or their residential environments substantially change. ...
... First, older people are sometimes overburdened by their housing costs, which constitute 35% of their household expenditures, and 43% of the expenditures of those in the lowest income quartile(Social Security Administration, 2013).These costs primarily include the rent and utilities of renters and the mortgage payments, property taxes, and property insurance of owners. In 2011, 61% of renters and 35% of homeowners age 65 and older paid more than 30% of their household incomes on these housing expenses. About 36% of renters and 18% of owners paid monthly dwelling costs that were more than 50% of their incomes(U.S. Department of Housing and Urban Development, 2013). ...
Resilience: thoughts on the value of the concept for critical gerontology
2
2013
... (1) 他们是更具灵活性的个体(Skodol, 2010; Aldwin et al, 2012; Wiles et al, 2012b; Wild et al, 2013).他们具有的个性、价值观和人口统计学特征(年龄、职业、文化、收入等)激励和帮助其找到创造性和建设性的自我适应策略来应对逆境.例如,他们可能有更丰富的技巧去解决问题,或丰厚财力使其更容易承担额外成本.这些老年人过去的生活经历使其更有能力解决遇到的问题.他们可能具有信任他人和开放的个性,容易得到别人帮助和支持,因此会积极寻求解决问题的方案.他们也可能是更快乐的人,对生活具有乐观的看法,从而对自己的未来更有希望. ...
... The theory proposes three factors to explain why some older people have more enriched coping repertories(Fig.4). First, they will be more resilient individuals(Skodol, 2010; Aldwin et al, 2012; Wiles et al, 2012b; Wild et al, 2013). They will have personalities, values, and demographics that motivate and enable them to find creative and constructive adaptive strategies to deal with their adversity. For example, they may have stronger problem-solving skills or have financial resources that make it easier for them to tolerate the collateral costs connected with implementing their coping solutions. The past life experiences of these older individuals will have better prepared them to deal with their problems. They are likely to have personalities predisposing them to finding solutions because they are more trusting and open to receiving the help or supports of others. They are also likely to be happier persons who have optimistic outlooks on their lives and are therefore more hopeful about their futures. ...
a. The meaning of “aging in place” to older people
3
2012
... 六组社会学或心理学因素可以帮助解释就地养老对老年人的强烈吸引力(Wiles et al, 2012a; Golant, 2015b).第一,老年人愿意呆在熟悉的环境中.在这里其对周围事物有更准确、更完整、更可靠的认知,在自己住所和邻里社区周围活动使其感到更有信心、更能应付自如.即使遭遇停电,他们在黑暗中也能在住所内安全地找到所需的东西;同样,他们很清楚社区商店、服务设施及交通路线的具体位置,因此能够以最少的脑力和体力消耗满足自己的日常需要.在熟悉的地方,有朋友跟他们分享愉快的经历,因此不太会感到孤独;并且,当在日常生活中遇到困难需要帮助时(比如想要搭便车去看病或者找人帮忙买东西)时,他们非常清楚该向谁求助.所以,他们会担心,如搬到一个新的社区,需要好几年时间才能重新建立起此类可靠的关系. ...
... Six sets of social or psychological factors help explain older people's strong attractions to their current places of residence(Wiles et al, 2012a, Golant, 2015b). First, older people want to remain in familiar environments. Here they have more accurate, complete, and reliable cognitive maps of their surroundings. Consequently, they feel more confident and competent navigating around their dwellings, neighborhoods, and communities. If they lose electrical power, even in the dark they can safely find things in their dwellings. Similarly, they have good knowledge of where the stores, services, and transportation routes are in their communities and can satisfy their everyday needs with minimal mental and physical energy. In their familiar places, they have friends to share enjoyable social experiences and thus are less likely to feel alone. They are also more aware of who they can count on when they need assistance with their everyday needs—whether getting a ride to their doctors or assistance with their shopping. These older people reason that it would take years for them to establish such reliable connections in a new community. ...
... The theory proposes three factors to explain why some older people have more enriched coping repertories(Fig.4). First, they will be more resilient individuals(Skodol, 2010; Aldwin et al, 2012; Wiles et al, 2012b; Wild et al, 2013). They will have personalities, values, and demographics that motivate and enable them to find creative and constructive adaptive strategies to deal with their adversity. For example, they may have stronger problem-solving skills or have financial resources that make it easier for them to tolerate the collateral costs connected with implementing their coping solutions. The past life experiences of these older individuals will have better prepared them to deal with their problems. They are likely to have personalities predisposing them to finding solutions because they are more trusting and open to receiving the help or supports of others. They are also likely to be happier persons who have optimistic outlooks on their lives and are therefore more hopeful about their futures. ...
b. Resilience from the point of view of older people: 'there's still life beyond a funny knee'
1
2012
... (1) 他们是更具灵活性的个体(Skodol, 2010; Aldwin et al, 2012; Wiles et al, 2012b; Wild et al, 2013).他们具有的个性、价值观和人口统计学特征(年龄、职业、文化、收入等)激励和帮助其找到创造性和建设性的自我适应策略来应对逆境.例如,他们可能有更丰富的技巧去解决问题,或丰厚财力使其更容易承担额外成本.这些老年人过去的生活经历使其更有能力解决遇到的问题.他们可能具有信任他人和开放的个性,容易得到别人帮助和支持,因此会积极寻求解决问题的方案.他们也可能是更快乐的人,对生活具有乐观的看法,从而对自己的未来更有希望. ...
The contributions of race, individual socioeconomic status, and neighborhood socioeconomic context on the self-rated health trajectories and mortality of older adults
2
2008
... 第五,邻里和社区发生的一些变化会令老年人感到不便.当一家喜欢的商店关闭、一位医生退休,或一条公共汽车线路停止服务,老年人就会感到自己的生活受到困扰.在一些没有活力的老城市、小城镇和农村,失去农业、制造业或能源领域工作的老年人经济上陷入困境.这些社区被称为“老人留守”的地方,因为年轻人口迁移别处寻求就业,留下的是失业的、受教育程度较低的人和老年人(Golant, 1984).这些地方可能出现社会秩序混乱(如犯罪、毒品、酗酒、破坏公物),建筑物废弃或破败.老年人一般会减少外出,因为独自外出缺乏安全感;并且,这些地方往往缺少休闲娱乐的条件(如公园、广场、图书馆和为老年人组织的活动),及保健和长期照护服务(Krause, 2003; Yao et al, 2008). ...
... Fifth, older people find themselves in neighborhoods and communities that have experienced undesirable physical or demographic changes. The lives of older people are disrupted when a favorite store closes, a doctor retires, or a bus service stops. Other communities—in older cities, small towns, and rural counties—decline economically because they have lost jobs in their agricultural, manufacturing, or energy sectors. Sometimes they are referred to as "aged left behind" localities, because younger populations migrate elsewhere seeking jobs and the unemployed, less educated, and older populations are left behind(Golant, 1984) . These places are more likely to have social disorders, such as crime, drug and alcohol use, and vandalism and have abandoned or physically rundown buildings. Older people in these locales tend to venture out less frequently, feel insecure walking alone, and they lack the supports of trusted neighbors. These places often lack recreational amenities(e.g., parks, public squares, libraries, and organized events for older people), but also healthcare and long-term care offerings(Krause, 2003; Yao et al, 2008). ...


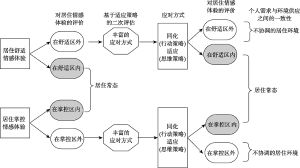

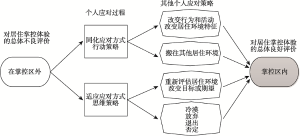


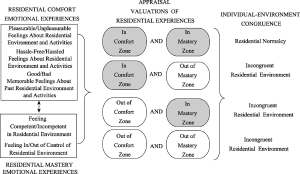


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}